An article written by Dr Edward Leatham, Consultant Cardiologist © 2025 E.Leatham
Introduction
Visceral adipose tissue (VAT) is a pro-inflammatory, metabolically active fat depot that plays a key role in the pathogenesis of hypertension, coronary heart disease (CHD), and atrial fibrillation (AF). Unlike subcutaneous fat, VAT resides deep within the abdomen and contributes to insulin resistance, endothelial dysfunction, and adverse cardiac remodelling¹.
Traditional risk markers like BMI fail to capture VAT burden. Instead, VAT index (VATI)—the VAT area in cm² indexed to body surface area (m²)—offers a precise, clinically meaningful target. Our practice applies gender- and ethnicity-specific VATI thresholds, such as <38 cm²/m² for Caucasian men and <28 cm²/m² for Caucasian women, with lower thresholds for Asian populations².
1. Screening with Waist-to-Height Ratio
The waist-to-height ratio (WHtR) is a simple and effective tool to flag individuals at higher risk of VAT accumulation. A WHtR ≥ 0.5 indicates increased cardiometabolic risk, even in patients with normal BMI³.
Why use WHtR ≥ 0.5?
- More accurate than BMI for central fat
- Quick, reproducible, and cost-free
- Valid across age, sex, and ethnic groups
- Especially valuable in identifying VAT in patients with non-diabetic hyperglycaemia (NDH)—defined as impaired fasting glucose or impaired glucose tolerance⁴
2. VATI Requires Imaging for Precision
Waist-to-height ratio is a better guide to VAT than BMI, but it still reflects both subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT). SAT is metabolically inert; VAT is inflammatory and strongly linked to cardiometabolic risk⁵. The waist circumference is a valuable tool to monitor changes in central adiposity over time. However, it cannot distinguish VAT from SAT. Therefore in order to accurately identify and track VAT, an imaging test—such as low-dose CT or MRI— may be essential. We use low-dose, single-slice CT at L3, which is:
- Highly reproducible
- Low in radiation
- Cost-effective for long-term monitoring⁶
For selected patients at risk, we establish baseline VATI assessment with an option for repeat assessment at 6 months, which supports decision-making around therapy escalation (e.g. GLP-1 receptor agonists) and validates response to lifestyle change.

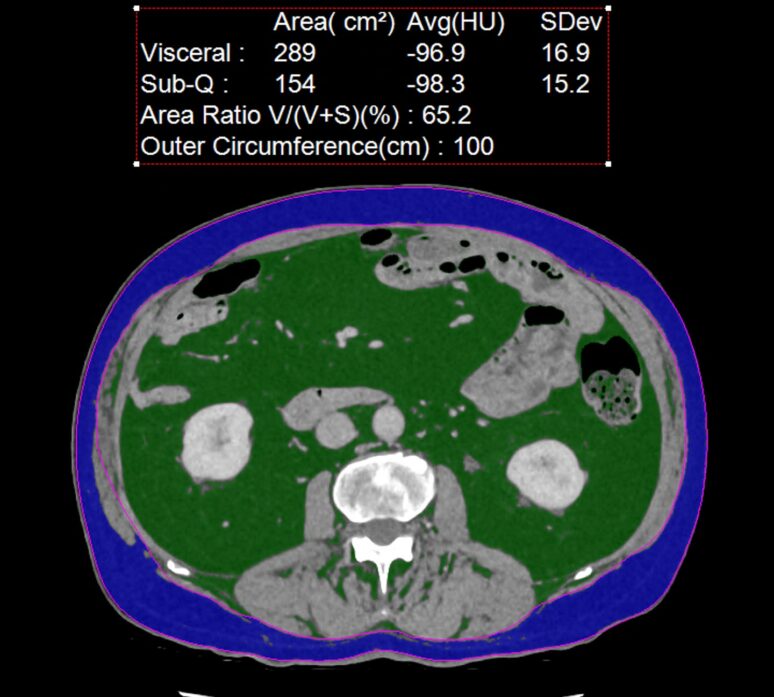
An example of a non contrast CT showing visceral adipose in green and metabolically inactive subcutaneous adipose tissue in blue. In this patient the VAT measures 289 cm2 which is over double recommended (100 cm2).
3. VATI Targets by Gender and Ethnicity
Using gender- and ethnicity-specific VATI thresholds improves sensitivity and specificity in identifying high-risk individuals:
| Ethnicity | Male VATI Threshold (cm²/m²) | Female VATI Threshold (cm²/m²) |
|---|
| Caucasian | <38.0 | <28.0 |
| South Asian | <34.0 | <25.0 |
| East Asian | <32.0 | <23.0 |
| Black | <36.0 | <26.0 |
| Hispanic | <36.0 | <27.0 |
| Other/Unspecified | <35.0 | <26.0 |
4. Digital Tools as Adherence Amplifiers
Lifestyle change works—but long-term success depends on adherence. Our program uses structured digital tools and personalised planning frameworks to support this journey.
1. Dr Shape Food Analysis App
Our patients are enrolled in Dr Shape, a clinical nutrition app programmed with their personal calorie and macronutrient goals. It acts as a real-time food bot, providing:
- Meal-by-meal feedback
- Macronutrient breakdowns and adjustments
- Goal tracking across the day
- Behavioural nudges to improve food choices
Patients use Dr Shape daily for at least 3 months, allowing precise, data-driven dietary guidance outside clinic settings.
2. Continuous Glucose Monitoring (CGM)
Used to identify those affected and to treat patients with non-diabetic hyperglycaemia (NDH) or insulin resistance, CGM is used to:
- Identify post-meal glucose excursions
- Tailor carbohydrate intake and timing
- Help prevent hyperglycaemia-driven VAT accumulation
3. Body Composition Scales and Waist Tracking
We encourage use of smart body composition scales to monitor:
- VAT estimates (where available)
- Lean mass retention
- Hydration status
Paired with weekly waist circumference, these tools help patients track their own progress and reinforce motivation between imaging assessments.
4. Optional Nutrigenomix DNA Testing
For selected patients—particularly those with metabolic resistance or micronutrient concerns—we offer Nutrigenomix DNA testing. This test identifies gene variants that affect:
- Protein requirements
- Lactose or fat sensitivity
- Caffeine metabolism
- Micronutrient metabolism (e.g. folate, B12, vitamin D)
This information helps tailor the dietary plan even further—e.g., lowering daily protein targets or advising folate-rich foods in those with MTHFR variants.
5. Tiered 6-Month VATI Intervention Pathway
Tier 1: Digital Lifestyle Program (First 6 Months)
Patients with VATI above target are invited to enter a 6-month lifestyle and dietary programme, gradually incorporating the following into a long term, sustainable lifestyle changes:
- Aerobic activity ≥150 mins/week
- Resistance training 2x/week or daily 10 min routine.
- HIITS 10-15 min 3 x each week
- Caloric targets with macronutrient goals via Dr Shape
- Digital adherence tools (CGM, smart scale, waist tracking)
After 6 months, VATI can be re-assessed via repeat CT or surrogate.
Tier 2: Add GLP-1 Receptor Agonist (If Target Not Met)
For non-responders (VATI remains ≥ threshold), or where there is a strong preference to intervene, GLP-1 receptor agonists are added:
- Proven to reduce VAT independently of weight loss⁷
- Improve insulin sensitivity and reduce hunger
- Recommended in high-risk patients by expert guidelines⁸
6. Follow-Up and Reassessment
Every 6 Months:
- CT VATI measurement
- Waist circumference and weight
- Smart scale body composition metrics
- (If hypertensive)
BP via Hilo BP band
- CGM in NDH patients
This structured follow-up ensures we track metabolic progress and tailor therapy only where needed.
Conclusion
VAT reduction is a clinically powerful and achievable goal. Our programme identifies high-risk patients using WHtR and imaging, and applies a tiered model of care centred around:
- Digital dietary support (Dr Shape)
- Real-time glucose tracking (CGM)
- Smart scales and waist tracking
- 6-month imaging reassessment
- GLP-1 therapy only in non-responders
This approach empowers clinicians and patients alike—delivering precision, avoiding overtreatment, and improving cardiometabolic outcomes.
References
- Fox CS, Massaro JM, Hoffmann U, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors. Circulation. 2007;116(1):39–48.
- Ashwell M, Gibson S. Waist-to-height ratio is a simple and effective screening tool for cardiovascular risk. Obes Rev. 2016;17(3):275–86.
- Alberti KG, Zimmet PZ. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia. Diabet Med. 1998;15(7):539–53.
- Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–8.
- Shen W, et al. Estimating body composition from a single CT image. Am J Clin Nutr. 2004;80(2):271–8.
- Baggerman MR, et al. Reference values for visceral fat by CT. Obesity (Silver Spring). 2023;31(1):12–21.
- Oh TJ, et al. GLP-1 RA and SGLT-2 inhibitors in VAT reduction. PLoS One. 2023;18(9):e0289616.
- Yum Y, et al. Expert consensus on hypertension management in obesity. Clin Hypertens. 2024;30(1):13.
Other related articles
- Anthropometrics vs BMI: Why Waist Measures Outperform BMI in Cardiovascular Risk Assessment
- Why everyone is talking about VAT
- How to Lose Visceral Adipose Tissue (VAT) and Improve Metabolic Health: A Guide to Sustainable Weight Loss
- The Expanding Waistline in Men: Spare Tyre, Killer Visceral Fat, or Just Flabby Abdominal muscles?
- From Genes to Greens: How DNA Shapes Your Nutritional Needs
- The 8-Month Metabolic Reset: A New Approach to Reversing Visceral Fat, Improving Blood Pressure and Blood Glucose