An article by Dr Edward Leatham, Consultant Cardiologist © 2024 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
In my first explanation of the normal functioning of the heart, much was made of the sucking action of the left ventricle as it relaxes between heart beats, a process that draws oxygenated blood into the heart from the lungs via its ‘antechamber’ the left atrium. A fraction of a moment later, the left atrium further assists left ventricular filling when its muscle lining contracts, just before each heartbeat, ‘priming’ the main pumping chamber, just like a turbocharger primes a petrol engine. The reason for this emphasis is that a failure of left ventricular priming with the atrium being rendered useless by AFib is an important cause of breathlessness in patients with atrial fibrillation and/ or aging, both of which are extremely common. It is therefore important and relevant to explain what is going on, so that patients and doctors can understand how to treat it. The topic is too extensive to cover in one session, so in this story, I’m simply going to cover the haemodynamics.
Think of the lungs as something like the “bilges” in a boat—an area that could flood if not properly managed. Just like a bilge pump clears out water from the boat’s hull, the heart’s left ventricle clears fluid from the lungs. If the heart stops, this “pump” shuts down, leading to flooding in the lungs. This is why, during a cardiac arrest, fluid quickly builds up in the lungs.
The left atrium, the chamber just above the left ventricle, is connected to veins from the lungs. When the pressure in the left atrium rises, even slightly, it can push fluid into the tiny air sacs in the lungs, which makes it harder for oxygen to pass from the lungs into the blood. This increased pressure explains why heart patients often feel breathless.
Several issues can raise the pressure in the left atrium, such as problems with the valve between the atrium and ventricle (called the mitral valve), or if the left ventricle becomes stiff and loses flexibility. As this pressure builds up, a substance called BNP increases in the blood, and doctors use BNP measurements, along with ECG readings, to understand why a patient may be struggling to breathe.
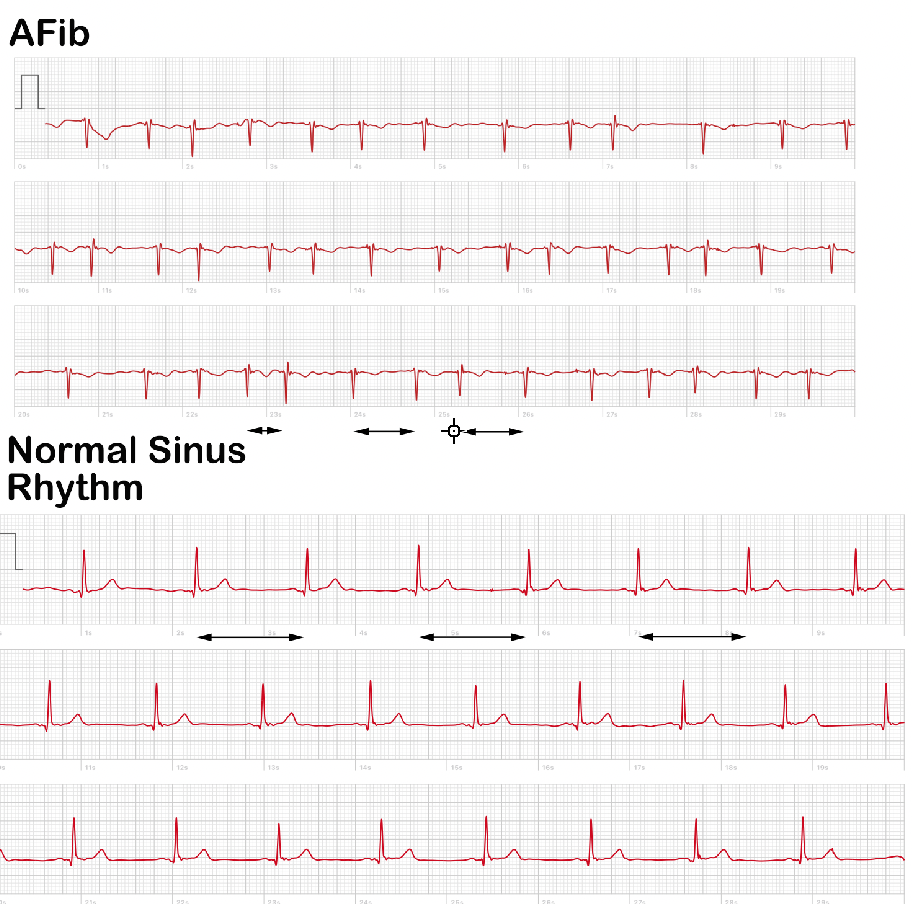
Now, in atrial fibrillation (AFib), the left atrium’s rhythmic contraction becomes erratic, no longer providing a steady flow of blood into the left ventricle. Instead, it just passively channels blood from the lungs to the ventricle. Without the atrial contraction helping to “prime” the ventricle, less blood may enter during the heart’s relaxation phase, which can lower the amount of blood the heart pumps out and increase pressure in the lungs. This situation can lead to fluid buildup in the lungs, making breathing more difficult—similar to how a car performs poorly if its turbocharger is failing.
In young, healthy hearts, the left ventricle is flexible, able to relax and “suck in” blood with ease. By the time the atrium contracts, the ventricle is almost full, so AFib often doesn’t cause noticeable issues in younger people. However, as people age or with conditions like high blood pressure or diabetes, the ventricle becomes stiffer, losing its ability to pull in blood naturally. In these cases, the atrium’s boost becomes essential, so AFib has a bigger impact.
A good analogy is an old leather bellows for a fire, which becomes harder to pull air into over time. Similarly, a stiffer left ventricle requires more effort from the atrium to fill properly. When doctors assess this using echocardiographythey use an “E:A ratio” to measure the blood flow pattern into the ventricle. In a flexible heart, blood flows easily, shown by a higher “E” (early filling) compared to “A” (atrial contraction filling). In a stiffer heart, this pattern reverses, showing that the atrium’s help is more critical to maintaining normal blood flow.
Timing
With atrial fibrillation, there is an additional problem of an increase in heart rate. The main thing the left ventricle need to fill is time, and if this time is restricted by an increase in heart rate, as tends to occur in atrial fibrillation, there is insufficient time in diastole for it to fill adequately.
In atrial fibrillation, there are therefore two reasons why breathlessness occurs. The first being the lack of atrial ‘kick’ or contraction to eject blood from the left atrium into the left ventricle prior to each heart beat, particularly if the left ventricle is stiffened with age, hypertension or poor glucose control. The second reason is that the interval between each heartbeat, or so-called ‘RR interval’, is reduced as the patient’s heart rate is increased in most people in atrial fibrillation, particularly when active and this compounds the problem further because there is insufficient time for sufficient blood to move from the left atrium and pulmonary veins into the heart for the next beat. The end result is that as the patient walks, or in some cases even at rest, the pulmonary venous pressures rise, the alveolar gas exchange is impaired, and the patient feels breathless. In severe cases, the bilge pumps fail and the bilges fill up, meaning that the patient is breathless at rest, especially on lying flat and the lung floods to the point it can even be seen on a chest X-ray as shadowing, and in extreme cases, as pleural effusions. This is called pulmonary oedema and can be diagnosed by listening to the lungs with a stethoscope and has typical appearances on a chest x-ray.
Its now, I hope easy to understand why many patients with atrial fibrillation cannot exercise as well as when they are in normal rhythm. This is one of the main reasons that cardiologists will tend to treat a patient with symptoms in atrial fibrillation by attempting to restore the normal rhythm.
This is why there is often a major benefit of restoring left atrial contractility and priming function of the heart in the elderly patient who has gone into atrial fibrillation who feels breathless. Although a second-line approach of simply lowering the heart rate, so-called rate control, is helpful, it is not as good as normal sinus rhythm or rhythm control.
Further reading
- Left Atrial Hypertension in Atrial Fibrillation: Dealing With the Pressure 2017
- What is Atrial Fibrillation (AFib)?
- What advice for patients at risk of AF?