With increasing awareness that atrial fibrillation (AFib) is extremely common, affecting up to 10% of people by the age of 70, it is important to address that for every one patient in persistent or permanent atrial fibrillation, there are dozens, if not hundreds, of patients who are having short periods of atrial fibrillation, lasting 30 seconds or more. Somewhat arbitrarily the medical professional defines periods of chaotic atrial rhythm last lasting less than 30 seconds ‘atrial ectopic runs‘ and those that last greater than 30 seconds ‘paroxysmal atrial fibrillation‘ or ‘PAF’ for short. So what advice do we have for our patient having frequent atrial ectopics and short runs showing on their ambulatory ECG where we know that in the long term, these may progress to more prolonged periods of atrial fibrillation, which they may not be fully aware of?
It is acknowledged that a patient needs to have more than 24 hours of continuous atrial fibrillation before there is any real risk of embolic complications that develop as a result of a thrombus growing within the left atrial appendage during periods of AF. Therefore, patients experiencing shorter periods of paroxysmal atrial fibrillation need not be too concerned. However, if they are not fully aware of their arrhythmia, there is a risk that it may progress over years to longer and longer periods until it can then present, sadly, with a devastating stroke. This, incidentally is why the UK Department of Health/NICE recommends that any patient with either Afib or PAF with a raised CHADVASC2 score of over 1 should consider taking anticoagulants.
With growing public awareness and knowledge, there is an understandable and increasing interest in patients employing self help techniques to look out for AF episodes. After all, it is hardly going to be possible to obtain an ECG from your GP every time you feel a slightly irregular pulse.
An important point to mention is that patients who start off having symptoms from their palpitation can gradually become accustomed to the arrhythmia and thus become less aware. So, someone who is fully aware of their palpitation when they first present may, five years later, be completely unaware as they slip into periods of AF lasting days, if not weeks. This is the largest risk group of patients, represented on most stroke wards, where for up to half of all patients who have devastating strokes, it’s their unrecognised AF that’s caused it.

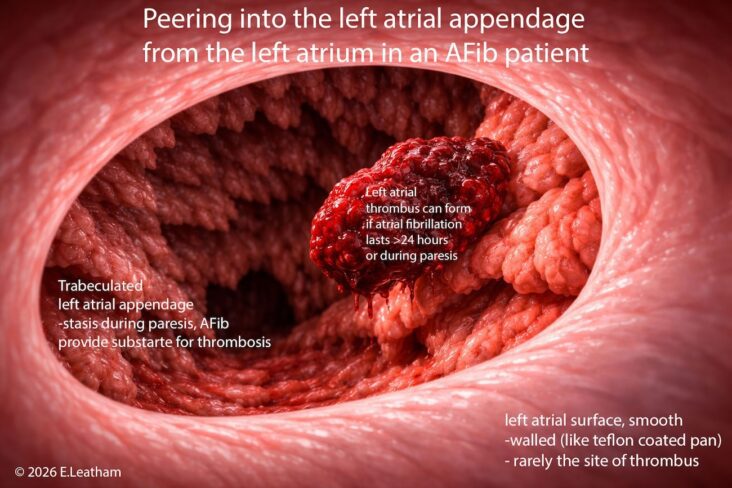
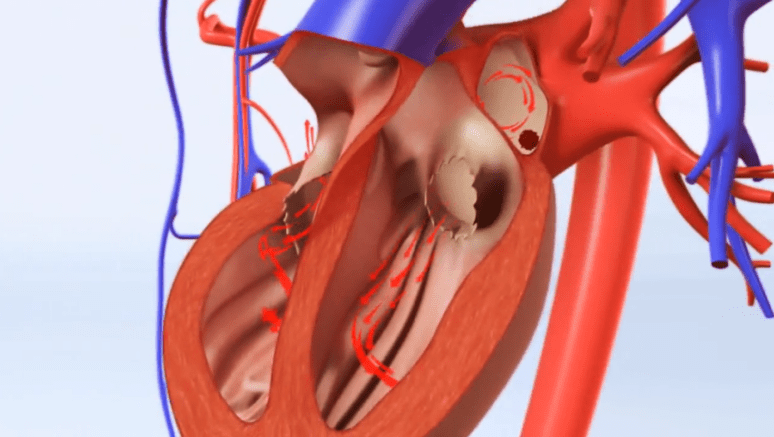
After 24 hours of continuous atrial fibrillation, unless anticoagulant drugs such as warfarin or a DOAC are being taken, a thrombus (clot) can form within the outpouching of the left atrium (the left atrial appendage).
In unfortunate cases, this can detach and float in the arterial circulation (embolism) impacting into medium size arteries of the brain, coronary tree, gut and limbs to cause; stroke, heart attack, ischaemic gut or critical limb ischaemia.
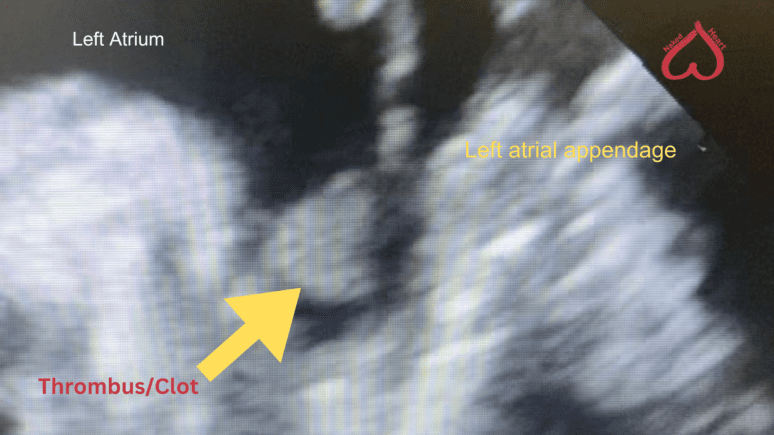
In this image we have capture such a clot using a transoesophageal echocardiogram (TOE) that allows the cardiologist to view the left atrial appendage from the gullet, since this area of the heart cannot be seen using the standard transthoracic echocardiogram
A simple hack worth knowing is that that a person’s resting heart rate is set by the balance of their sympathetic and vagal tone, so will, unless ill or taking drugs, vary very little from day to day. In AFib, the resting heart rate WILL change in most people increasing by at least 10 bpm over their normal resting heart rate and in some cases can be be super fast – up to 180 BPM. Just by tracking heart rate, a person can thus can an idea of whether their heart is in AFib.
The techniques that we recommend for patients to monitor themselves are various, including a pulse check each morning as part of a routine. This is particularly straightforward for anyone who is or has been a healthcare professional, as they have been trained early on in their careers to do a pulse check. It is, however, simple enough for anyone to learn how to take their own pulse using online material.
The second simple method is to use a simple pulse oximeter, which shows the arterial waveform in a small display. It’s quite easy to see whether there is an erratic pulse, as well as obtain an accurate pulse rate with these instruments, which cost on the order of £25.
Another non-ECG method that is widely used, and in fact often a reason for referral to a cardiologist, is the Fitbit, as this monitor checks the regularity of the pulse and gives the pulse rate over 24 hours. Many of the manufacturers of these devices now have built-in algorithms that warn patients if the pulse rates are inappropriately high or are irregular, suggesting that there may be atrial fibrillation present.
The ECG App – such as Alivecor turns your smart phone into a heart rhythm recorder which allows you to take a recording at home at any time, and get a professional interpretation if the inbuilt diagnostics give ambiguous results.
For the more discerning customer, the ECG watch, which is worn most of the time, is an obvious choice. It combines the technology used by the Fitbit device to oversee the general heart rhythm, with the option to take a formal heart rhythm recording by touching the crown of the watch and creating a circuit that allows a good quality rhythm strip, etc., to be taken and recorded onto your smartphone. Many of the manufacturers now have reporting platforms that can be used if the automated reporting software is inadequate, and there are blog articles on this website to help people discern whether their ECG strip is showing signs of atrial fibrillation as well.
The two devices that we have experience with are the Apple Watch and the Withings Watch. The latter looks more like a traditional watch and has fewer features (e.g., you can’t answer a telephone call on it or pay for goods using Apple Pay). However, it does have the advantage of having a battery life of nearly a month, so it requires less charging as opposed to the Apple Watch, which needs to be charged daily. For those worried that their AF may occur at night, the Apple Watch can be charged in just a few hours, so it’s best charged in the early evening and then worn overnight to catch any nocturnal arrhythmias that may be occurring.

 After 24 hours of continuous atrial fibrillation, unless anticoagulant drugs such as warfarin or a DOAC are being taken, a thrombus (clot) can form within the outpouching of the left atrium (the left atrial appendage).
After 24 hours of continuous atrial fibrillation, unless anticoagulant drugs such as warfarin or a DOAC are being taken, a thrombus (clot) can form within the outpouching of the left atrium (the left atrial appendage).
 The ECG App – such as Alivecor turns your smart phone into a heart rhythm recorder which allows you to take a recording at home at any time, and get a professional interpretation if the inbuilt diagnostics give ambiguous results.
The ECG App – such as Alivecor turns your smart phone into a heart rhythm recorder which allows you to take a recording at home at any time, and get a professional interpretation if the inbuilt diagnostics give ambiguous results.