An article by Dr Edward Leatham, Consultant Cardiologist © 2025 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
Cardiovascular disease (CVD) – encompassing strokes, heart failure, coronary artery disease, and sudden cardiac death – remains the leading cause of death globally. While many associate heart disease with advancing age, the reality is that CVD often begins its insidious course decades before symptoms arise. By the time chest pain, breathlessness, or a heart attack occur, the underlying pathology has usually been progressing silently for years.
Despite this, most national prevention strategies primarily target individuals over the age of 60, relying heavily on calculated 10-year cardiovascular risk thresholds. This age-centric approach, while pragmatic from a public health standpoint, often misses younger individuals who carry significant modifiable risk factors. Tragically, for many patients, the opportunity for truly preventative intervention is long past by the time formal risk assessments are triggered.
The uncomfortable reality is that cardiovascular prevention efforts frequently offer “too little, too late.” Many men aged between 40 and 60 – a critical period often referred to as “Sniper’s Alley” – suffer fatal heart attacks, often without prior symptoms or warning. Perhaps the general awareness of premature death toll in men also contributes to why many ‘at risk women’ are so often ignored, with the result that more women than men die of CVD due to systemic under treatment at all ages. Education and earlier, more proactive strategies could prevent many of these events.
Public understanding is beginning to shift. Increasing numbers of people in their 20s and 30s are now seeking information about how to safeguard their cardiovascular health proactively. Over the next six weeks, I will be releasing a series of blog articles offering a cardiologist’s perspective on prevention measures to be considered in each age group <20, 20-30, 30-40, 40-50, 50-60 and over 60 yr, with practical advice on how individuals can engage their healthcare teams to develop personalised risk-reduction strategies.
This first article sets the scene, exploring why early prevention matters, why family history significantly alters the approach, and how the latest science is changing our understanding of cardiovascular risk – especially the crucial role of lifetime exposure to low-density lipoprotein cholesterol (LDL-C).
The Types of Modifiable Risk Factors
Modifiable risk factors are those that individuals can influence through lifestyle changes, medical management, or both. They broadly include:
- Raised LDL cholesterol (LDL-C) and other lipid abnormalities
- High blood pressure
- Tobacco smoking
- Mental health issues and poverty that exacerbate poor lifestyle and dietary factors
- Inflammatory conditions such as untreated rheumatoid and psoriasis
- Untreated viral infections including HIV
- Obesity and waist-height ratio abnormalities
- Poor diet, particularly high saturated fat and processed carbohydrate intake
- Physical inactivity
- Raised lipoprotein(a) (LP(a)), although not directly modifiable yet, is important to recognise
- Type 2 diabetes and insulin resistance
Critically, all these factors interact over time. The longer an individual is exposed to elevated LDL-C, high blood pressure, obesity, and smoking, the greater the cumulative damage to the arterial walls. The earlier risk factors are identified and managed, the greater the potential to prevent irreversible atherosclerotic changes.
Why Family History Matters
When considering cardiovascular risk, family history is a powerful indicator that can substantially modify the preventive approach. Specific questions cardiologists ask include:
- Has a first-degree relative (parent, sibling, or child) experienced a heart attack, coronary stenting, or bypass surgery under the age of 60?
- Has a close relative suffered a stroke, or developed significant hypertension, atrial fibrillation, or an aortic aneurysm at a relatively young age?
- Are any relatives diagnosed with Familial Hypercholesterolaemia (FH) or prescribed statins from a young age?
- Are there any relatives diagnosed with raised LP (a)?
If the answer to any of these is ‘yes,’ the patient’s baseline cardiovascular risk is elevated, often regardless of their current lifestyle. This necessitates an earlier, more aggressive screening and prevention programme.
The Evolution in Approach: Lifetime LDL Burden
Historically, most prevention strategies were based on predicting an individual’s 10-year risk of a heart attack or stroke. This is still reflected in many guidelines today. However, the science of cardiovascular prevention has evolved significantly in recent years.
There is now overwhelming evidence that lifetime exposure to elevated LDL-C is a primary driver of atherosclerotic cardiovascular disease (ASCVD). Even modestly elevated LDL-C, if left untreated from a young age, can lead to a heavy cumulative burden of arterial plaque by midlife.
Lowering LDL-C earlier in life is dramatically more effective at preventing cardiovascular disease than waiting until risk scores trigger treatment thresholds at age 60 or later. Once plaque has formed, risk can be reduced but never completely eliminated – a concept termed the “cholesterol years hypothesis.”
This shift in understanding underpins the growing enthusiasm for early lipid screening, particularly in individuals with a family history of heart disease, and supports earlier initiation of LDL-C lowering therapies where appropriate.
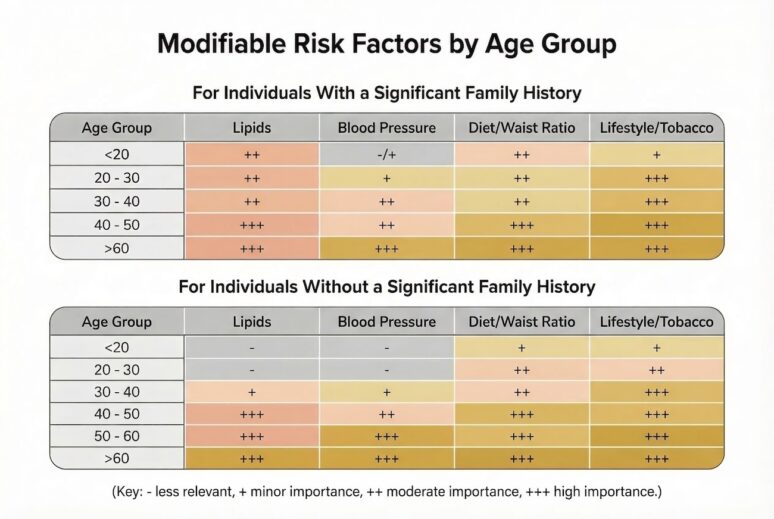
Modifiable Risk Factors by Age Group
The importance of different risk factors varies by age and family history. Below is a summary based on clinical frameworks increasingly used by cardiologists:

These tables illustrate why earlier assessment and intervention is critical for those with ‘significant’ family histories. In clinical practice, a “significant family history of heart disease” usually refers to premature atherosclerotic cardiovascular disease (ASCVD) in a first-degree relative.
Standard definition (most commonly used)
- First-degree relative (parent, sibling, or child) with:
- Myocardial infarction (MI)
- Coronary revascularisation (PCI/stent or CABG)
- Sudden cardiac death presumed cardiac
At a premature age:
- <55 years in males
- <65 years in females
Screening Guidelines and Advice on prevention
For Those With No Significant Family History:
- Maintain a healthy weight and physical activity levels.
- Routine cardiovascular screening (lipid profiles, blood pressure checks) typically begins at 40.
- Focus on lifestyle optimisation and smoking cessation.
- Basic cardiac evaluation (e.g., ECG, echocardiography) considered for competitive athletes.
For Those With a Significant Family History:
- Initiate lipid profile testing in the late teens or early 20s.
- Strong consideration for advanced lipid testing, including LP(a) levels.
- Regular blood pressure monitoring from young adulthood.
- Waist-height ratio and metabolic markers assessed early.
- Setting of individual key health metrics with follow-up at intervals to track changes and interventions such as lipid lowering, healthy metabolism and weight over time.
Special Focus: Inherited Lipid Disorders
Familial Hypercholesterolaemia (FH):
- Affects 1 in 250 people.
- Leads to very high LDL-C from birth.
- Associated with premature coronary artery disease if untreated.
- UK NICE guidelines recommend cascade testing of first-degree relatives.
- Statin therapy from a young age can normalise life expectancy when started early.
Raised LP(a):
- Present in about 20% of the population.
- Potent, independent risk factor for atherosclerosis and valve disease.
- Currently no specific therapies are available, but screening identifies individuals who need more aggressive LDL-C lowering.
Other Critical Modifiable Factors
Smoking:
- Remains a leading preventable cause of heart disease.
- Particularly dangerous when combined with elevated LDL-C or diabetes.
Obesity and Waist-Height Ratio:
- Central obesity is a major driver of metabolic syndrome and cardiovascular risk.
- A waist-to-height ratio above 0.5 signals early risk and should trigger intervention.
Diet:
- Excess processed carbohydrate and saturated fat intake accelerates atherosclerosis.
- Lifelong dietary habits strongly influence cardiovascular outcomes.
Physical Inactivity:
- Regular exercise halves the risk of coronary heart disease compared to sedentary individuals.
- Activity guidelines recommend at least 150 minutes of moderate-intensity exercise per week.
- Endurance events such as iron man and marathons add no extra benefits over regular cardiovascular exercise, and indeed carry small risks in individuals with unrecognised underlying heart conditions.
Conclusion: Early Action Saves Lives
Cardiovascular disease is not an inevitable consequence of ageing; it is largely preventable with early identification and management of risk factors. Lifetime exposure to raised LDL-C, poorly controlled blood pressure, central obesity, and smoking are the major determinants of who will develop atherosclerotic disease.
Those with a significant family history of early cardiovascular events must be especially vigilant. Early lipid screening, lifestyle modifications, and, where appropriate, pharmacological interventions can dramatically reduce future cardiovascular events.
Waiting until age 60 to begin prevention efforts is often far too late. The best time to act is now – whether you are 20, 30, 40, or beyond.
The coming articles will break down prevention strategies by age group, providing a roadmap to better cardiovascular health across the decades.
Key messages
- When it comes to coronary heart disease, LDL Cholesterol is considered to be the main determinant of the build up in coronary plaque that occurs in about 50% of our population by the age of 60. Coronary plaque is the first of four processes that lead to a heart attack.
- If you have raised LDL, dietary changes alone are unlikely to lower LDL sufficiently to prevent the build up of coronary plaque, causing atherosclerosis.
- If your LDL cholesterol exceeds 4.9 mmol/L and one or more relatives affected by heart disease (<60), then you should see your GP to discuss the possibility of familial hypercholesterolemia.
For other stories related to cholesterol, coronary heart disease, and LDL, explore the archives by entering a tag under the search function above.
Other related articles
- The Rise of Online Home Blood Testing: A Paradigm Shift in Preventative Healthcare
- LDL: the lower the better
- Cholesterol measuring 2024 guidance
- The latest ESC and locally developed guidelines on LDL targets
- Familial Hypercholesterolaemia NHSE