Despite large numbers of trials with evidence of effect, whether to take lipid lowering therapy remains oddly controversial. Atherosclerosis, the narrowing of blood vessels causing events, such as heart attacks or strokes, or slower damage, such as vascular dementia, is effectively impossible in the absence of cholesterol. Being born with almost no circulating cholesterol (or reduction of LDL to zero by drugs) results in nothing except a zero-lifetime risk of atherosclerosis (or cessation and reduction in atherosclerosis).
However, there is perhaps an understandable reluctance to use widespread medications; from an individual’s point of view to take drugs, the cost, the inconvenience, and the risk (or perceived risk) of side effects, and from healthcare’s point of view being able to afford to treat large numbers of people (both drug cost and people resource). There is also perhaps the opinion that atherosclerosis is caused by lifestyle choices and therefore populations should reduce their risk by changing their lifestyle e.g. smoke less, be thinner, exercise more. Although these are not unimportant risk factors, social deprivation and many other medical and genetic risk factors contribute significantly so it is incorrect and unfair to assume that lifestyle choices cause all heart attacks and that lifestyle modification will obliterate the risk. Cardiovascular risk is now the biggest killer of people in the world, and the UK, killing more women than men (despite male sex being a risk factor for atherosclerosis).
LDL or ApoB
Irrespective of what your risk may be due to, e.g. smoking, genetic conditions, inflammatory diseases, reduction of LDL (a lipid particle dense in cholesterol) has been shown to be effective at reducing the risk. One point of confusion is that the risk reduces proportionally with apoB (a protein found on various lipid particles but >90% on LDL) but historically the only drugs we had to reduce apoB were LDL reducing agents. Therefore some trials had unexpected results likely based on whether the lipid particle they were reducing included apoB or not. Measurement of apoB would significantly increase the cost of lipid testing and as we have never had a drug historically that reduced the number of all apoB containing particles, just LDL, there has not been the need to.
To take or not to take
The consideration to take lipid lowering therapy really comes down to the individual. For each person ideally you would want to know your risk of cardiovascular events, and your approach to risk. Ethically speaking you could also consider justice, i.e. the impact of your action on society.
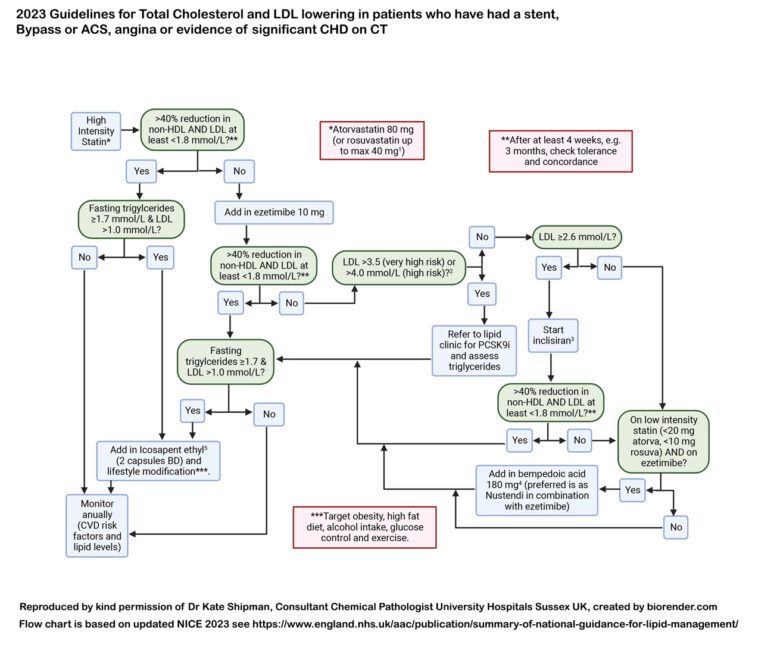
If we consider personal risk in the first place, this is extremely difficult to assess, particularly for people yet to have an event. If you already have evidence of atherosclerosis, particularly severe or significant, it is easy to know your risk, i.e. it is high. Therefore for people after a heart attack, or stroke, or symptomatic with leg claudication or angina then the risk is very high and we would normally recommend aggressive risk modification. LDL/ApoB lowering can reverse the atherosclerosis, proportionately to how much lowering one achieves. This must be combined with modification of all other risk factors that can be identified, e.g. smoking cessation. See the figure below for a very simple schema suggesting how to approach lipid lowering escalation. It is important to note that decisions do not need to be this binary but it is an attempt to demonstrate the eligibility criteria for patients in England under NHS care.
For those without any evidence of atherosclerosis it becomes much more complex. Risk calculators exist but are flawed when the data is used to inform an individual. You can look at your family history and you can identify significant risk factors e.g. diabetes mellitus and smoking. However even in families with high genetic risk from a single gene mutation, each individual can present at very different ages if untreated, demonstrating how variable the risk is. There are more than 200 risk factors. Effectively if we want to stop atherosclerosis we would give everyone an LDL of zero (although of course we would also promote healthy lifestyle and obliterate poverty). This would end up treating people with no risk in their lifetime i.e. those who would have lived to 102 years old with no medications, or be dead much younger from other causes. However if we consider the justice argument, keeping people well, working, independent, and out of residential care settings is of significant benefit to society, as well as reducing the significant human costs of the impact of disease on the individual and their friends and family.
Due to the fact that reducing LDL in everyone would work (and is even economically favourable) NICE in 2023 recommended that anyone with an informed personal preference to take a statin is eligible to have one. This is the first time you do not need to have proven high risk. This gets round the inaccuracy of risk prediction. However we are now left with the last thing to consider, your personal approach to risk. It is perhaps simpler after a heart attack, or stroke for example, if you want to live and stay well then lower your lipids. For some people however they may select a palliative approach and therefore appropriately avoid preventative therapy. If you are well with no known atherosclerosis and you are worried about your lifetime risk of atherosclerosis and its complications, then lower your lipids. Side effects are extremely rare and reversible, unlike significant end organ damage due to a stroke for example. Treatment is not necessarily for life, as when you are no longer interested in pursuing longevity you can stop the treatments but the legacy benefits (of having reduced/avoided atherosclerosis build up) will last for decades.
In conclusion, apoB lowering does reduce atherosclerosis and its complications at a rate proportional to the degree of reduction. Your approach to starting lipid lowering therapy is more complex than discussed but the decision will include knowing your risk, your approach to risk, and considering both the personal impact and impact of your illness or death on those around you. It is important to note that lipid lowering therapy is very well tolerated and effective (particularly statins) and that increasingly we have more classes of drug (so for the very few who would like treatment but struggle to tolerate one class of drugs this should only be the beginning of the treatment pathway).