An article by Dr Edward Leatham, Consultant Cardiologist. The opinions expressed in this article are entirely mine and not those of SCVC or a consensus view.
Coronary artery disease (CAD) is an inflammatory condition, a fact that forms the cornerstone of understanding and treating this pervasive illness. It’s long been known that a significant proportion of patients with CAD may have no symptoms, yet have signs of the disease detectable on EBCT and Multislice CT scans many years before any symptoms manifest. This realisation has fueled the widespread use of coronary artery calcification (CAC) scores as a predictive tool for future cardiovascular events. CAC has been instrumental in guiding clinicians to initiate preventive strategies, such as the early use of statins, particularly in primary prevention. Invasive and more recently CT-based coronary angiography have also been the gold standard for identifying coronary narrowing – the end result of chronic inflammation: calcified and noncalcified plaque. Coronary plaque, whether lodged within the walls of the coronary arteries or obstructing them, can lead to significant symptoms such as angina and acute coronary syndromes. However, all of these imaging methods of assessment only identify the visible aftermath of a process that has been simmering for years.
The Evolution of Coronary Risk Assessment
The latest advancements in technology and knowledge have unveiled that years before calcification occurs in the coronary arteries, non-calcified plaque can be detected. In fact, it can take many years of inflammation and healing for non calcified plaque to calcify and some patients (particularly women under 60) with substantial plaque disease, do not exhibit any coronary calcification at all. This crucial finding has prompted many clinicians specialising in preventative care to opt for a formal CT angiogram (using contrast) rather than relying solely on CAC score, especially in younger patients where there is concern about underlying atherosclerotic disease despite a low CAC score.
For those focused on prevention, the earlier a preventive strategy is adopted in at-risk patients, the more effective it tends to be. Consequently, there has been a growing interest in finding a technology that can detect inflammatory processes that precedes plaque formation detectable by the human eye on contrast CT. Additionally, there has been a need for a technique that can monitor the effectiveness of anti-atherosclerotic interventions, such as statins, in patients with established coronary artery disease, whether they have undergone stent placements, bypass operations, or have a history of coronary syndromes. Understanding whether the disease remains active is crucial, as persistent inflammation puts patients at risk of recurrent cardiovascular events.
The CaRi Heart Score: A Breakthrough in Predictive Technology
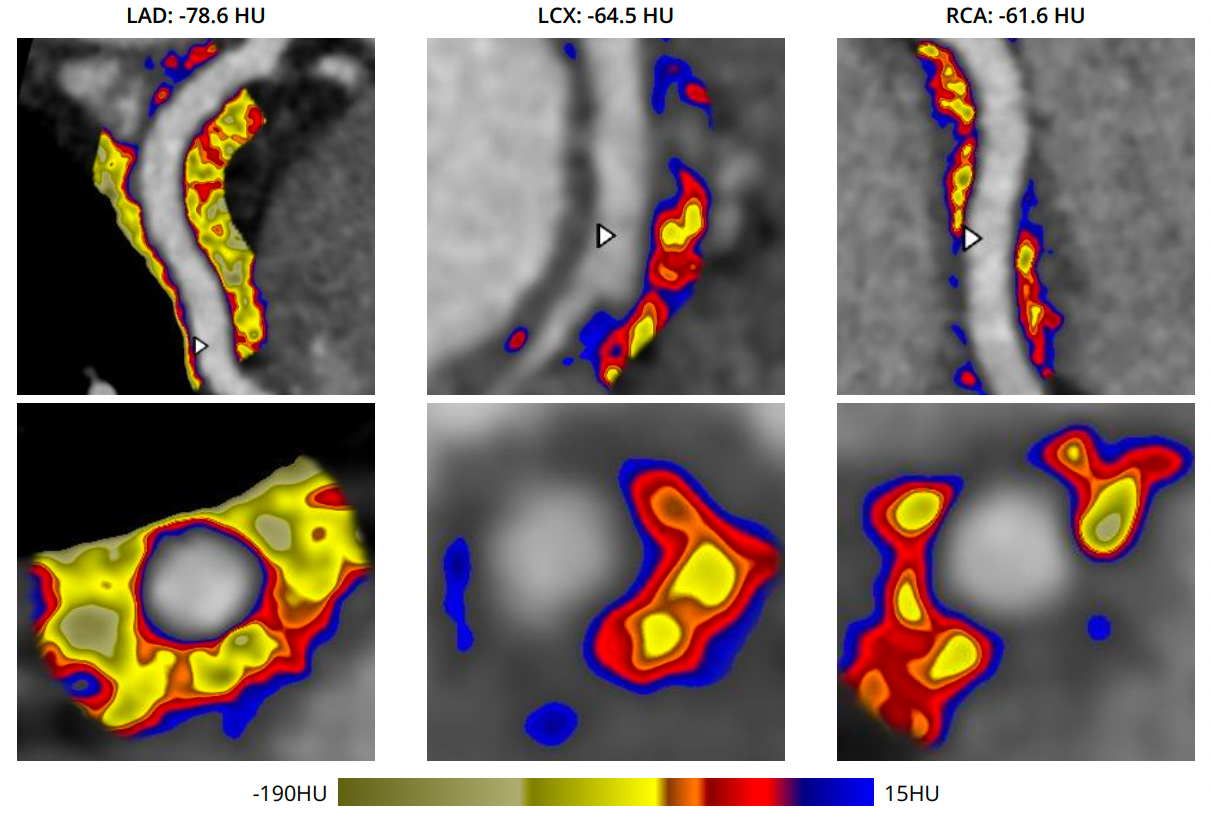
Decades of research from Oxford University led to the development of a novel technology that appears to meet these needs. The research, which has since been commercialized by the Caristo Group in Oxford, was groundbreaking in its use of radiotranscriptomic techniques to assess coronary artery inflammation [1]. By analysing signals present around the coronary arteries, the Oxford group was able to correlate these signals with inflammation in the coronary arteries, as demonstrated in coronary specimens taken from patients undergoing heart surgery. This paved the way for a non-invasive method to assess inflammation in the coronary arteries which was then used in large patient CTCA cohorts in North America and Germany to create an algorithm that predicted risk of fatal heart attack within 8 years. The technology is now encapsulated in what is known as the CaRi Heart Score, a test that is gaining traction among cardiologists with an interest in preventive strategies worldwide. The CaRi Heart Score leverages artificial intelligence and advanced imaging techniques to provide a more comprehensive assessment of coronary inflammation, even before non calcified and calcified plaque becomes detectable.
Interpreting the CaRi Heart Score: Navigating New Terrain
Despite its promise, the CaRi Heart Score has introduced some confusion, particularly due to the centile system used in its reports, which differs from the system traditionally used in CAC scoring. Many clinicians have observed that a majority of their patients score above the 50th centile in the CaRi Heart Score, a stark contrast to the distribution seen in CAC scores. While there are undoubtedly sound statistical reasons for this difference, it’s important to understand and recognize this disparity to avoid overestimating disease severity.
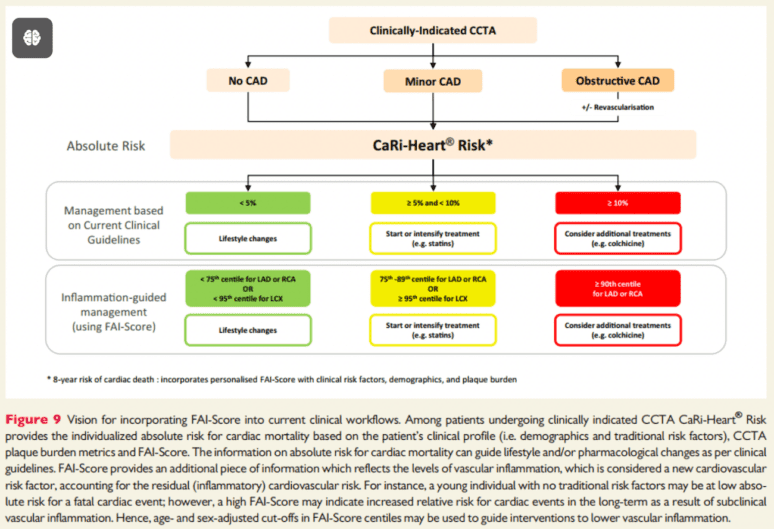
The publication, linked below [2], offers a comprehensive guide on how to manage and interpret these results. The paper includes a valuable table summarising the risk associated with inflammation in different coronary arteries, (shown below). Notably, it highlights the lower risk associated with inflammation in the left circumflex artery (LCX) compared to the right coronary artery (RCA) and the left anterior descending artery (LAD). This is an important consideration, as the model used in the CaRi Heart Score has not yet adjusted for coronary dominance—a factor that could significantly influence the interpretation of results. For instance, inflammation in a non-dominant RCA may not carry the same risk as in a dominant RCA, given that a non-dominant RCA can occlude without causing symptoms.
Clinical Application of the CaRi Heart Score
For now, cardiologists can use the CaRi Heart Score to tailor preventive strategies for each individual patient. In our advanced cardiovascular assessments, patients with high risk CaRi Heart Scores, placing them at intermediate or high risk, are offered a detailed metabolic health assessment where of all potentially modifiable risk factors, including LDL Cholesterol, ApoB, Lp(a), and glucose dysregulation are measured in addition to traditional lipid markers like LDL and apolipoprotein B. As expected the predominant ‘baddie’ associated with raised FAI is ApoB and raised LDL Cholesterol, however we are also finding a significant number of patients that have other previously unrecognised conditions that could be relevant to coronary inflammation including hypertension, elevated Lp(a), elevated homocysteine levels and glucose dysregulation. For patients with advanced disease some have multiple causes.
A comprehensive assessment allows for more aggressive preventive treatment that includes statins and PCSK9 inhibitors, lifestyle and dietary changes and for some of those at highest risk, referral to weight management consultant for GLP-1 agonist treatment. In a small subset of patients, particularly those at very high risk without an obvious key risk factor to target, we also utilise anti-inflammatory medications such as colchicine, which has been licensed for the reduction of coronary disease following interventional trials.
The use of AI-guided technology, such as the CaRi Heart Score, is revolutionising the way we approach cardiovascular prevention, enabling us to identify and mitigate risk factors before they manifest as clinical disease.
Future Directions and Considerations
As we continue to integrate the CaRi Heart Score into clinical practice, it is important to remain vigilant about the limitations and nuances of this new technology. The interpretation of results, particularly concerning coronary dominance and the percentile system, requires careful consideration to avoid mismanagement. However, the potential of the CaRi Heart Score to enhance our understanding of coronary inflammation and its role in cardiovascular disease cannot be overstated.
In conclusion, the CaRi Heart Score represents a significant advancement in the field of cardiovascular risk assessment. By detecting inflammation early and allowing for the tailored application of preventive strategies, this technology holds the promise of reducing the burden of coronary artery disease on a global scale. As with any new tool, ongoing research and clinical experience will be crucial in refining its use and maximizing its potential benefits for patients worldwide.

Conventional versus suggested use of FAI to risk stratify Cardiovascular Research, Volume 117, Issue 13, 15 November 2021, Pages 2677–2690, https://doi.org/10.1093/cvr/cvab286
Further Reading
- Can we use AI to predict cardiovascular death?
- A novel machine learning-derived radiotranscriptomic signature of perivascular fat improves cardiac risk prediction using coronary CT angiography
- Standardized measurement of coronary inflammation using cardiovascular computed tomography: integration in clinical care as a prognostic medical device 2021
- Inflammatory risk and cardiovascular events in patients without obstructive coronary artery disease: the ORFAN multicentre, longitudinal cohort study 2024
- Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease: JACC Review Topic of the Week 2023