An article written by Dr Edward Leatham, Consultant Cardiologist © 2024 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
In more than half of those affected with coronary artery disease (CAD) the first sign of the disease is an unprovoked heart attack or sudden death. Cardiologists have therefore been using cardiac CT for many years to identify patients at risk by assessing the extent, distribution, degree of vessel narrowing and calcification of coronary artery atherosclerotic plaque. Recently, formal long term follow up studies have confirmed the value of the cardiac CT angiogram (CCTA ) over and above standard risk calculators such as Q Risk.
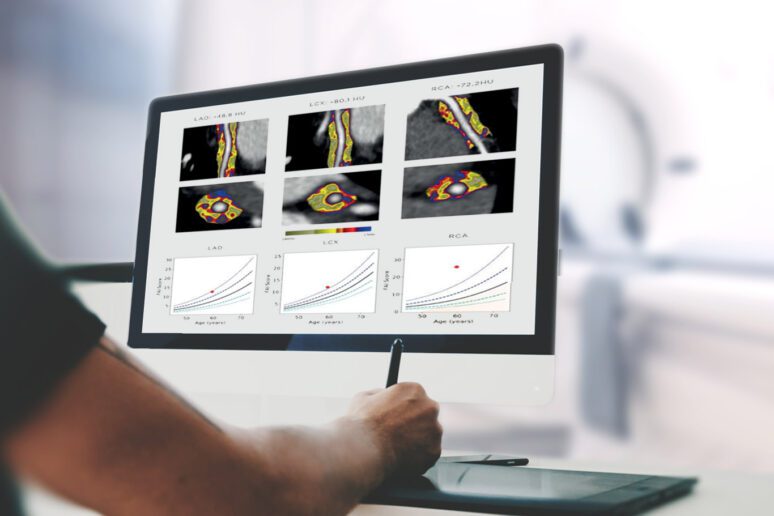
However, groundbreaking research from Oxford University reveals that it has recently also become possible to detect and quantify ‘coronary inflammation’ – considered to be a key driver of coronary heart disease, that can be found long before plaque and CAC show up on a standard CCTA. Since coronary inflammation is invisible to the human eye on conventional CT images, it requires artificial intelligence (AI) techniques to analyse the CT grey scale data to quantify inflammation which can then be presented in a simple metric known as the fat attenuation index (FAI). Computer modelling can than be used to predict risk of fatal heart attack. The late breaking news [1, 2] from AHA which hit the UK press in Nov 2023 clearly demonstrated that among thousands of patients undergoing CCTA, the majority of fatal and non-fatal cardiac events could have been better predicted using FAI, and occurred predominantly in those who did not have obstructive CAD at the time of imaging. Specifically, there were twice as many heart attacks and cardiac deaths in the group without obstructive CAD versus those with obstructive CAD.

Since early intervention is crucial in preventing heart disease, identifying individuals with high FAI (active coronary inflammation) earlier in the natural history of their coronary heart disease, allows us to target more effective prevention measures to those at highest risk.
At SCVC the consultation rooms and data stores are set up beside our own inhouse cardiac CT scanner so that results and AI data processing can be reviewed during the consultation.
Not everyone with risk factors for CHD has raised CaRi heart scores – the additional information gained from assessing FAI allows a tailored approach to prevention measures.
- The CaRi Heart Score: A New Frontier in Cardiovascular Risk Assessment
- https://www.prnewswire.co.uk/news-releases/american-heart-association-late-breaking-science-presentation-reveals-majority-of-adverse-cardiac-events-occur-among-patients-without-obstructive-coronary-artery-disease-but-risks-are-detectable-by-novel-ai-301986476.html
- Cardiovascular computed tomography imaging for coronary artery disease risk: plaque, flow and fat
- Assessing Cardiovascular Risk by Using the Fat Attenuation Index in Coronary CT Angiography