
This article explains how iron underpins oxygen delivery and cardiac energy production, why anaemia forces the heart to increase its stroke volume, and how that compensatory rise in cardiac output can generate a systolic murmur — even across a structurally normal aortic valve.
01 — THE PROBLEM Breathlessness Is Not Always a Heart Problem
When a patient arrives unable to climb a hill without stopping, the clinical instinct — theirs and ours — turns immediately to the heart. Could it be a blocked coronary artery? A failing valve? A clot on the lung? These are the right questions to ask, and they deserve prompt, systematic answers. But sometimes the diagnosis sits in a completely different compartment of physiology: the blood itself cannot carry enough oxygen.
Iron deficiency anaemia is one of the most prevalent conditions worldwide, and one of the most underestimated in cardiovascular medicine. It does not announce itself dramatically. It creeps — fatigue first, then breathlessness on exertion, then a heart that must work harder and faster simply to keep tissues oxygenated. Left untreated for long enough, it generates a heart murmur in patients who never had one before, and can make a mildly narrowed aortic valve appear far more severely diseased than it truly is.
This is the story of how that happens — from the chemistry of iron in the haem molecule, through the cellular machinery of cardiac energetics, to the haemodynamics of a compensating heart and the turbulent flow that produces the murmur a cardiologist hears through the stethoscope.
02 — OXYGEN TRANSPORT The Red Cell’s Only Job — and Iron’s Central Role
The red blood cell is the most specialised cell in the human body. It has surrendered its nucleus and its mitochondria to maximise the space available for a single purpose: transporting oxygen from the lungs to every tissue that needs it, and returning carbon dioxide in the other direction.
At the heart of this function is haemoglobin — the iron-containing protein that accounts for approximately 97% of a red cell’s dry weight. Each haemoglobin molecule consists of four protein chains (the globins), each wrapped around a haem group. At the centre of each haem group sits a single atom of iron in the ferrous (Fe²⁺) state. It is this iron atom that forms a reversible bond with oxygen as blood passes through the pulmonary capillaries, and releases that oxygen to tissues where local oxygen tension is low.
One red blood cell carries approximately 270 million haemoglobin molecules. Each haemoglobin molecule can bind four oxygen molecules — one per iron atom. The arithmetic of oxygen delivery in a healthy person is extraordinary. When iron is depleted, that arithmetic fails.
Haemoglobin
The oxygen carrier — four haem groups per molecule, each with one iron atom. Requires iron to function. Measured as g/L; the standard clinical index of anaemia severity.
Serum Iron & TIBC
Iron availability — serum iron reflects circulating iron; TIBC reflects transferrin’s unsaturated binding capacity. Together they define the degree of iron depletion.
Transferrin Saturation
The delivery index — the percentage of transferrin carrying iron. Below 15% indicates iron-restricted erythropoiesis. Below 10% signals severe deficiency.
Ferritin
Iron stores — reflects total body iron reserve. The earliest marker to fall in developing iron deficiency, before haemoglobin is yet affected.
03 — ANAEMIA Why Iron Deficiency Reduces the Red Cell Count
Iron is not merely a passenger on haemoglobin — it is the rate-limiting ingredient for red cell production. The bone marrow manufactures roughly 200 billion new red cells every day. Each requires haemoglobin, and haemoglobin requires iron. When iron stores are depleted, the marrow cannot produce enough haemoglobin to fill the cells it is making. The result is a population of red cells that are small (microcytic) and pale (hypochromic), carrying far less oxygen per cell than normal.
As older red cells die over weeks and months and are replaced by these iron-poor newcomers, the total oxygen-carrying capacity of the blood falls. Once haemoglobin drops below about 100 g/L, most people begin to notice something is wrong. Below 80 g/L, the body is in genuine physiological stress — and the cardiovascular system must mount a compensatory response.
Iron Beyond Haemoglobin
Iron does far more than build haemoglobin. It is an essential co-factor for cytochrome enzymes in the mitochondrial electron transport chain — the machinery that generates ATP in every cell. Heart muscle cells (cardiomyocytes) are among the most mitochondria-rich cells in the body, running almost entirely on oxidative phosphorylation. In severe iron deficiency, even correcting the anaemia with a blood transfusion leaves cardiac cells functionally impaired — still starved of the iron they need to generate energy efficiently. This is why intravenous iron improves exercise capacity and symptoms in heart failure patients even when haemoglobin is only mildly reduced.
04 — CARDIAC COMPENSATION How the Heart Responds to Falling Oxygen Delivery
The body’s response to anaemia is rapid, elegant, and ultimately unsustainable without treatment. When oxygen delivery falls, chemoreceptors and tissue hypoxia signals drive the autonomic nervous system to increase both heart rate and — crucially — stroke volume: the volume of blood ejected with each beat.
This compensatory rise in stroke volume is achieved through the Frank-Starling mechanism. The heart fills more completely during diastole, ventricular walls stretch further, and that stretch translates into a more forceful systolic contraction. Cardiac output — the product of heart rate and stroke volume — rises to compensate for the reduced oxygen content of each millilitre of blood.
For a time, this compensation is effective. Breathlessness appears only on significant exertion. As anaemia deepens, the compensation fails to keep pace, and symptoms emerge at lower and lower levels of activity. The heart is now under sustained haemodynamic stress: a hyperdynamic, overworked chamber generating dramatically higher flow velocities across the cardiac valves with every beat — and this is where the murmur enters the picture.
Why Severe Anaemia Produces a Heart Murmur
Heart murmurs arise when blood flow becomes turbulent rather than laminar. Turbulence is governed by the Reynolds number — a function of flow velocity, vessel radius, and blood viscosity. In significant anaemia, two of these three factors shift simultaneously in the direction of turbulence: flow velocity rises (because stroke volume has increased) and blood viscosity falls (because the red cell count is low — the blood is literally more dilute and watery).
The result is a soft, blowing, systolic murmur — typically loudest at the left sternal edge or pulmonary area — in a patient whose aortic and pulmonary valves may be structurally completely normal. This is called a flow murmur or haemic murmur. It is not a sign of structural valve disease. It is a direct sign of the haemodynamic stress the anaemia is imposing on the heart. It resolves when the haemoglobin is corrected.
A critical clinical corollary: in a patient with known mild aortic stenosis, significant anaemia drives up stroke volume and therefore the velocity of blood across the already-narrowed valve. The transvalvular gradient rises, the murmur becomes louder and harsher, and echocardiographic grading may classify the stenosis as moderate or even severe. This is a diagnostic trap. Always correct haemoglobin before making definitive judgements about aortic stenosis severity — the true degree of stenosis will only be apparent once the hyperdynamic state has been resolved.
05 — CASE A Patient Who Arrived Breathless — and Left with Answers
A woman in her eighth decade presented with new-onset breathlessness on hills and palpitations over the preceding few weeks, following a long-haul flight and a brief illness abroad. She had also noticed some leg cramping and mild swelling in the days before presentation, which had reasonably raised concern about a possible deep vein thrombosis and pulmonary embolism — a legitimate clinical worry in the context of recent extended travel.
On examination she appeared well, without clinical signs of deep vein thrombosis. Blood pressure was reassuringly normal. The chest was clear. However, there was a soft systolic murmur audible at the left sternal edge — the kind of quiet, blowing sound that in this context warranted careful explanation rather than dismissal.
An immediate D-dimer was low, effectively excluding clinically significant active thrombosis. BNP was normal for her age, making cardiac failure very unlikely. A pulmonary embolism and new coronary event were both considered and set aside with confidence. The 12-lead ECG was completely normal.
Her blood tests told a very different story:
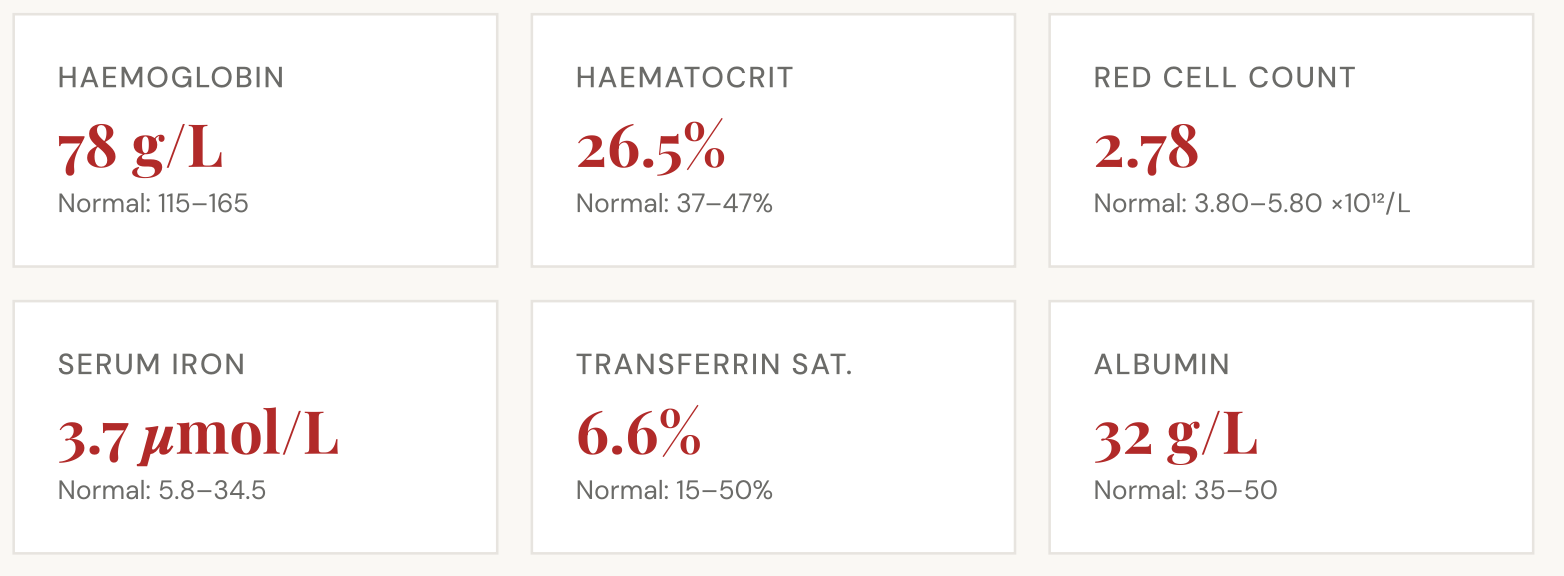
This was not mild iron deficiency. A haemoglobin of 78 g/L with a transferrin saturation of 6.6% represents severe, established iron depletion. The murmur was immediately explained: her heart had been compensating for months of progressively falling oxygen delivery by driving up its stroke volume, and the resulting turbulent, high-velocity flow across an otherwise structurally normal aortic valve was producing exactly the soft systolic murmur we heard through the stethoscope.
The cause of the iron deficiency — whether from occult blood loss, malabsorption, or a combination — required investigation as a matter of clinical urgency. Given a family history of colorectal cancer and recently worsening dyspepsia, she was referred for upper and lower GI endoscopy alongside intravenous iron therapy to correct the deficiency rapidly. The breathlessness, the palpitations, and the murmur are all expected to resolve as her haemoglobin recovers to normal levels.
06 — IRON AT CELLULAR LEVEL Why Iron Matters Far Beyond the Red Cell
It is easy to think of iron deficiency purely as a haematological problem — too little iron means too little haemoglobin means too few red cells. But iron’s biological role is considerably broader, and its effects on the heart operate at a cellular level that transcends the red cell count entirely.
Mitochondrial Electron Transport
Cytochrome c, cytochrome oxidase (Complex IV), and the Rieske iron-sulphur protein (Complex III) all require iron as a structural and redox co-factor. Without adequate iron, ATP synthesis in cardiomyocytes is impaired regardless of oxygen supply.
Myoglobin
Cardiac and skeletal muscle contain myoglobin — a single-chain haem protein that stores oxygen intracellularly and releases it rapidly during high-demand contraction. Iron depletion reduces myoglobin, stripping the heart of this critical intracellular oxygen buffer.
Ribonucleotide Reductase
This iron-dependent enzyme is essential for DNA synthesis and therefore for the bone marrow’s ability to produce new red cells. Iron deficiency impairs the very mechanism the body needs to correct itself — a self-perpetuating cycle.
The Clinical Implication
Because iron is essential for mitochondrial function in cardiomyocytes independent of its role in haemoglobin, correcting anaemia with a blood transfusion does not fully restore cardiac energetics. The iron deficiency itself must be treated. This is why intravenous iron therapy — not transfusion alone — is the correct primary intervention in iron deficiency anaemia presenting with cardiac symptoms, and why IV iron has been shown to improve exercise capacity in heart failure patients even when anaemia is mild.
07 — INVESTIGATION Iron Deficiency Is Never a Diagnosis in Itself
Confirming iron deficiency anaemia answers the question of mechanism. It does not answer the question of cause — and that question is always mandatory.
In younger women, menstrual blood loss and dietary inadequacy are the most common explanations. In older patients, particularly those with GI symptoms, new or worsening dyspepsia, or a family history of bowel cancer, the threshold for upper and lower GI endoscopy must be low. Colorectal cancer, gastric cancer, peptic ulceration, angiodysplasia, and coeliac disease are all causes that carry their own treatment implications and prognoses entirely separate from the anaemia they produce.
NSAID use — common in older patients managing musculoskeletal pain — is a frequent and often underappreciated contributor to upper GI blood loss. It is worth asking specifically about recent increased NSAID use in any patient presenting with new iron deficiency anaemia, particularly where GI symptoms have worsened in parallel.
Clinical Note — Investigation Sequence
Where iron deficiency anaemia is confirmed, the standard investigation sequence in an adult without an obvious dietary explanation is: (1) ferritin, serum iron, TIBC, and transferrin saturation to confirm the diagnosis; (2) coeliac serology (anti-tTG IgA with total IgA); (3) upper and lower GI endoscopy in patients over 50, or in younger patients with GI symptoms, family history, or unexplained deficiency; (4) intravenous iron to correct the deficiency rapidly while investigation proceeds — oral iron is often poorly tolerated and corrects slowly.
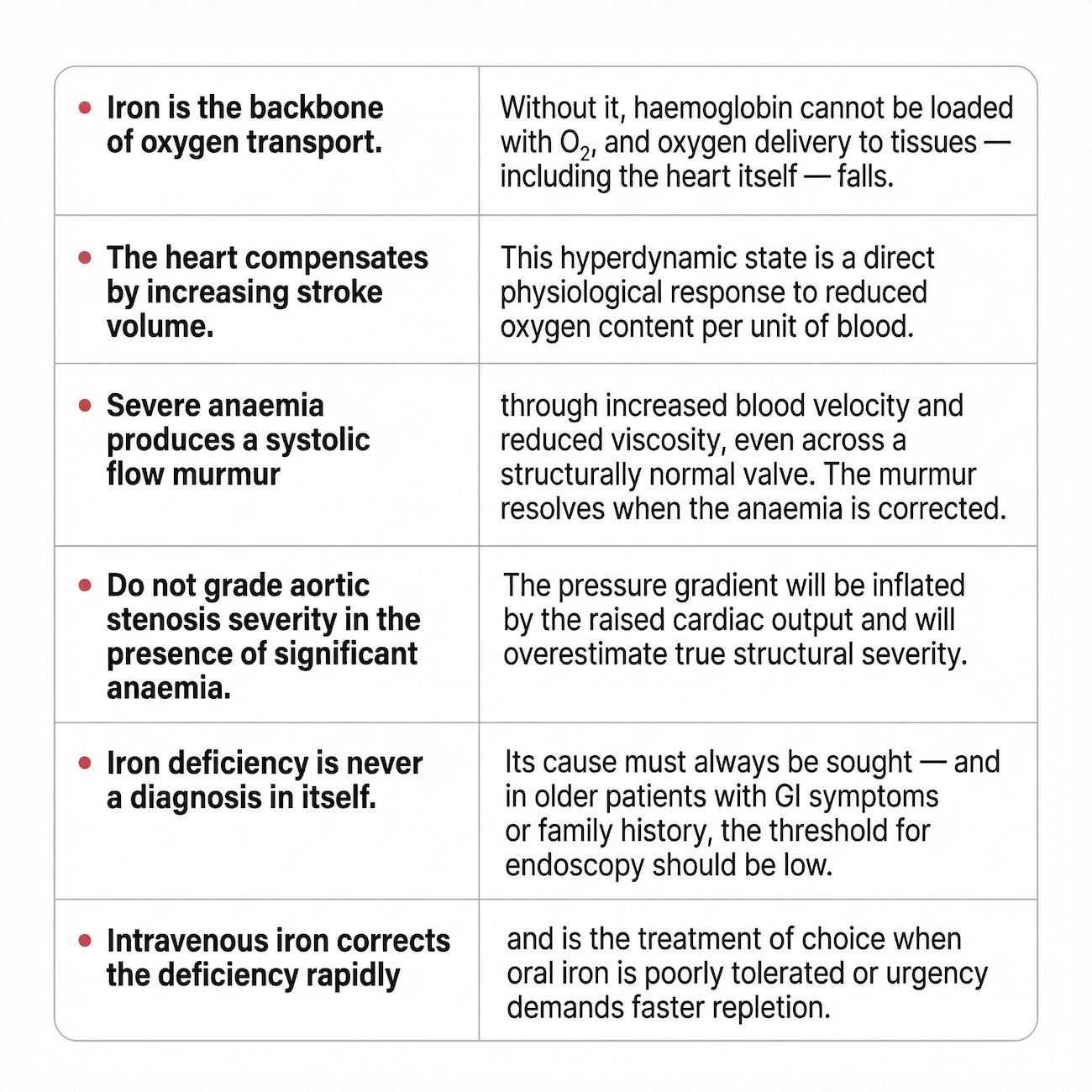
Take-Home Messages for Patients and Clinicians
Disclosure: This article is part of The VAT Trap educational series by Dr Edward Leatham and is intended for educational purposes for patients and clinicians. It does not constitute individual medical advice. The clinical case described has been anonymised with all identifying details removed. Patients with new breathlessness, palpitations, or a new heart murmur should seek clinical assessment promptly. All treatment decisions should be made in partnership with a qualified healthcare professional.



