An article by Dr Edward Leatham, Consultant Cardiologist © 2026 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
This blog is for people who have a diagnosis of atrial fibrillation or atrial flutter – especially if it is paroxysmal or persistent.
The Common Assumption
Patients diagnosed with atrial fibrillation (AF) who have a low CHA₂DS₂-VASc score (0–1) are often reassured that their risk of stroke is minimal. In many cases, this is correct when considering long-term stroke prevention. For more information about this group and CHA₂DS₂-VASc calculator see separate blog
However, there is an important and often underappreciated exception:
👉 The period surrounding cardioversion
Even patients with otherwise low stroke risk may face a transient but clinically significant risk of thromboembolism when AF is terminated—whether spontaneously or with medical intervention.
Understanding the Mechanism: Atrial Paresis
When atrial fibrillation or atrial flutter terminates and normal sinus rhythm is restored, the electrical rhythm may normalise immediately—but the mechanical function of the atrium does not recover instantly.
This temporary impairment is known as atrial paresis (also referred to as atrial stunning).
During this phase:
- The atrium contracts weakly or not at all
- Blood flow becomes sluggish, particularly within the left atrial appendage (LAA)
- Conditions favour local thrombus (clot) formation
Crucially, this occurs despite a normal ECG rhythm.
This disconnect between electrical recovery and mechanical recovery is the key reason why stroke risk persists after cardioversion.
The Left Atrial Appendage: A High-Risk Zone
The left atrial appendage is a small, pouch-like structure arising from the left atrium. Under normal conditions, it contracts effectively and prevents blood stagnation.
However, during AF—and especially during atrial paresis:
- Blood flow becomes static
- The appendage acts as a reservoir for clot formation
- Thrombi formed here can embolise to the brain or systemic circulation
It is well established that the majority of AF-related embolic strokes originate from the left atrial appendage.
Why Duration of AF Matters
The duration of atrial fibrillation prior to cardioversion is one of the most important determinants of thromboembolic risk.
Short Duration AF (<24 hours)
- Lower likelihood of clot formation
- Shorter duration of atrial paresis
- Often considered lower risk
Prolonged AF (>24 hours)
- Increased likelihood of thrombus formation within the LAA
- More prolonged and pronounced atrial dysfunction after cardioversion
- Higher risk of embolic events
👉 This means that even a young, otherwise low-risk patient may be at significant stroke risk if AF persists beyond 24 hours.
⚠️ Key Clinical Insight
A low CHA₂DS₂-VASc score reflects baseline stroke risk, but it does not account for transient high-risk periods, such as:
- AF lasting longer than 24 hours
- Cardioversion (any type)
- The period of atrial paresis following rhythm restoration

1. Natural (Spontaneous) Cardioversion
This occurs when the heart restores normal sinus rhythm without medical intervention.
Common triggers include:
- Viral illness
- Alcohol excess (“holiday heart syndrome”)
- Acute stress or inflammation
Most episodes resolve within 24 hours, particularly in younger patients. However:
- In older individuals or during prolonged illness, AF may persist longer
- Episodes exceeding 24 hours carry increased thromboembolic risk
2. Chemical Cardioversion
This involves the use of medications to restore sinus rhythm.
Common agents include:
- Amiodarone
- Flecainide (in selected patients)
These are typically administered under medical supervision and may act over hours to days.
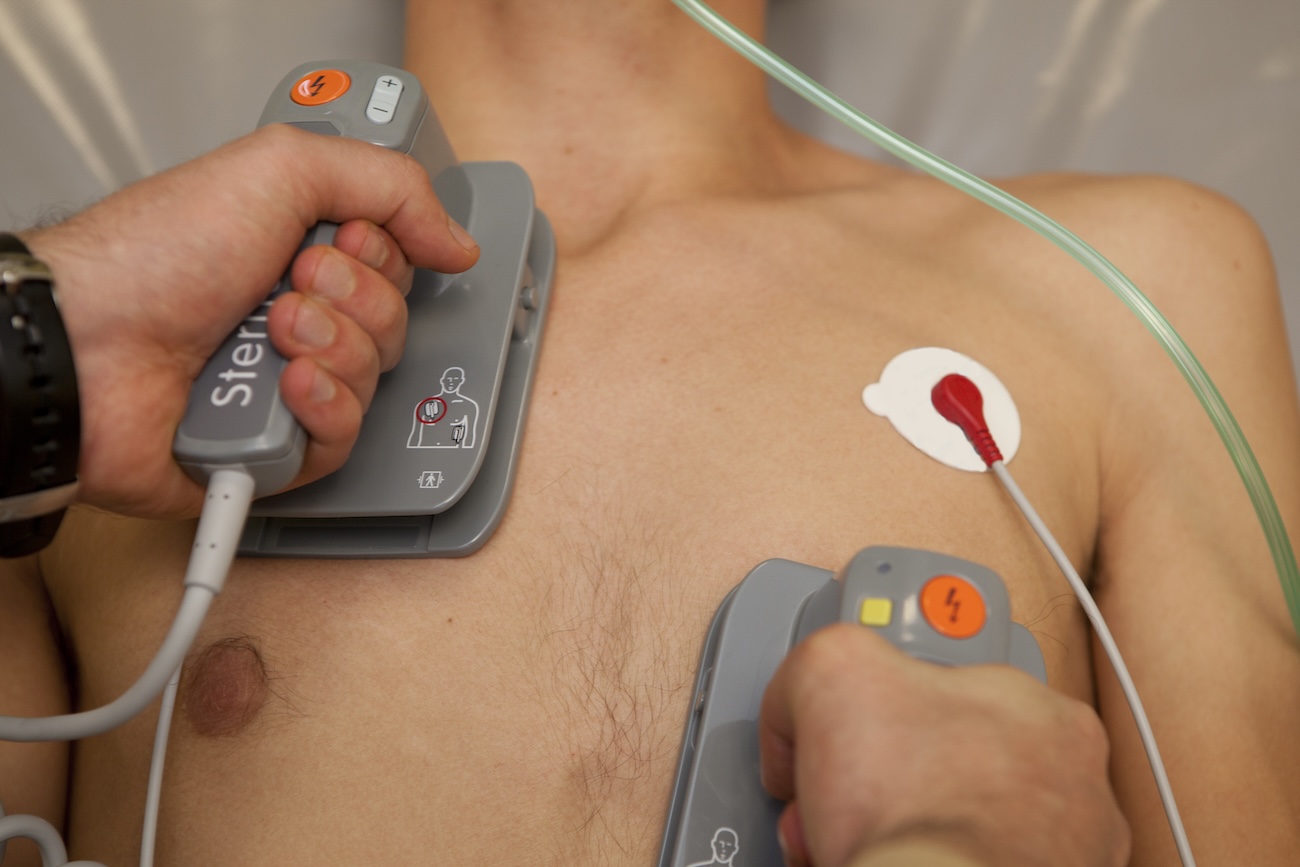
3. Electrical (DC) Cardioversion
This is the most direct and controlled method.
- Performed in hospital
- Requires light sedation or anaesthesia
- A synchronised electrical shock restores sinus rhythm
✅ Critical Point:
Atrial paresis occurs after all forms of cardioversion, including spontaneous conversion.
Anticoagulation Around Cardioversion
When AF or atrial flutter has been present for more than 24 hours, there is a risk that thrombus may already have formed within the left atrium.
Standard Practice
- Anticoagulation for 3–4 weeks prior to cardioversion
- Continuation for at least 4 weeks after cardioversion
This approach reduces the risk of dislodging pre-existing thrombus and prevents new clot formation during atrial paresis.
Role of Transoesophageal Echocardiography (TOE)
In certain cases, a TOE (transoesophageal echocardiogram) can be used to visualise the left atrial appendage directly.
- If no thrombus is detected, immediate cardioversion may be performed
- However, anticoagulation is still required after the procedure due to atrial paresis
View a different blog to see what a left atrial appendage thrombus looks like on TOE
Why Anticoagulation Continues After Cardioversion
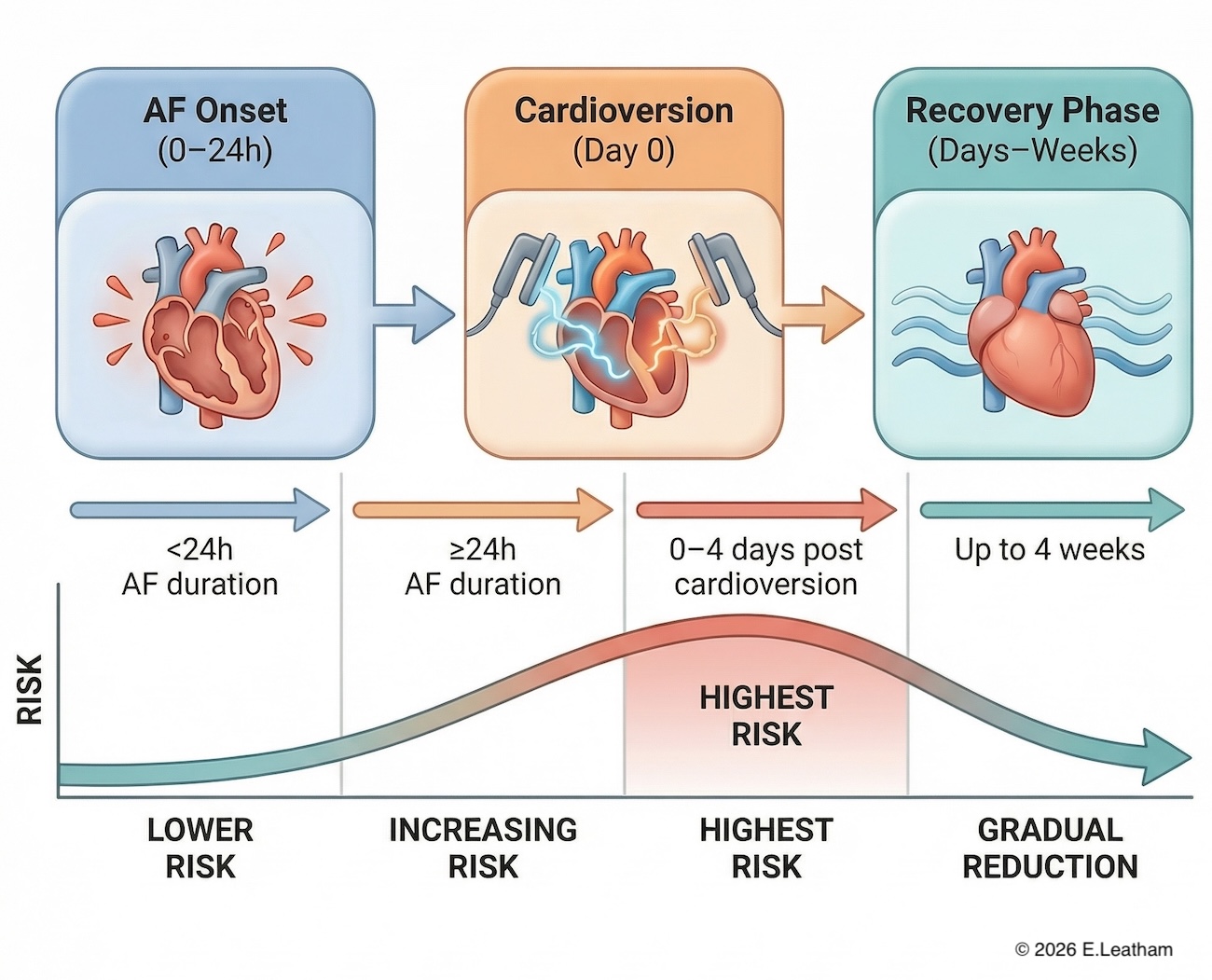
The period immediately following restoration of sinus rhythm is particularly important.
Peak Risk Window
- Highest risk occurs during the first 3–4 days
- Risk remains elevated for up to 4 weeks
This reflects:
- Ongoing atrial mechanical dysfunction
- Continued stasis within the LAA
👉 Importantly, this risk exists even if the patient feels well and ECG is normal.
Warfarin and Anticoagulation Targets
For patients treated with warfarin:
- INR should be >2.5 at the time of cardioversion
- INR should remain therapeutic (>2.0–3.0, ideally >2.5) for at least 3–4 weeks afterwards
For patients on direct oral anticoagulants (DOACs), adherence and correct dosing are essential.
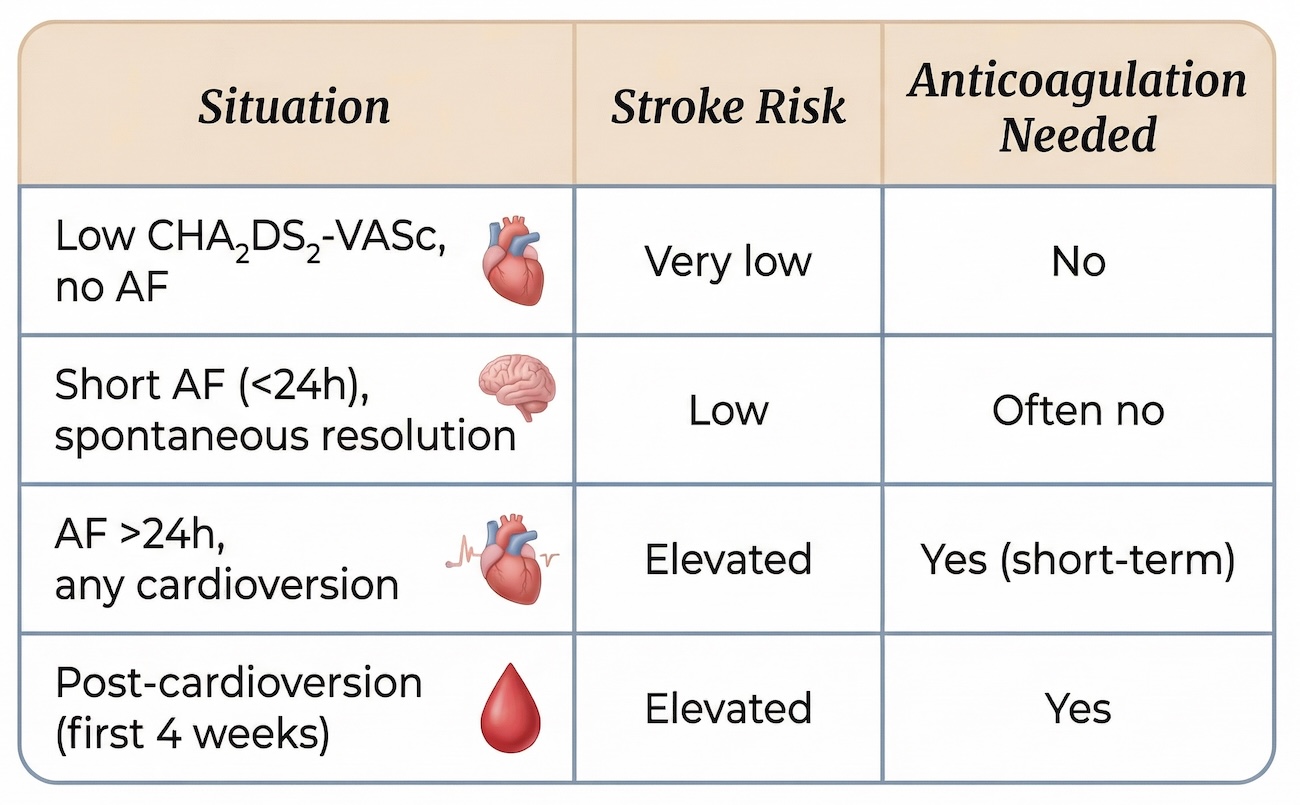
Implications for Low-Risk Patients
Patients with a low CHA₂DS₂-VASc score are often not anticoagulated long-term. However:
👉 This does not apply during the peri-cardioversion period
Key points:
- Stroke risk becomes procedure- and timing-dependent
- Even a single prolonged episode of AF can carry risk
- Anticoagulation is temporary but essential in many cases
Putting It All Together
A practical way to understand this:
Key Take-Home Messages
- A low CHA₂DS₂-VASc score does not eliminate short-term stroke risk
- Atrial paresis is a critical and often overlooked phenomenon
- AF lasting more than 24 hours significantly increases risk, regardless of baseline score
- All forms of cardioversion carry a temporary thromboembolic risk
- Anticoagulation before and after cardioversion is essential in these situations
Final Thought
Stroke prevention in atrial fibrillation is not simply about long-term risk scoring.
👉 It is also about timing, physiology, and atrial recovery
Recognising the role of atrial paresis ensures that even low-risk patients receive appropriate short-term protection during vulnerable periods.
Key References
- European Society of Cardiology (ESC) Guidelines for the diagnosis and management of atrial fibrillation
https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Atrial-Fibrillation - National Institute for Health and Care Excellence (NICE) Atrial fibrillation: diagnosis and management
https://www.nice.org.uk/guidance/ng196 - American Heart Association / American College of Cardiology / Heart Rhythm Society AF Guideline Update
https://www.ahajournals.org - Manning WJ et al. Left atrial appendage function after cardioversion (atrial stunning)
https://pubmed.ncbi.nlm.nih.gov/ - Cardiac Electrophysiology review on atrial stunning and thromboembolism risk
https://www.ncbi.nlm.nih.gov/
Related Blogs
- Two ways AFib can cause stroke or heart attack
- What is Atrial Fibrillation (AFib)?
- Managing your own Atrial Fibrillation: Taking control of your heart health
- How AFib can present as a heart attack or stroke