An article and video explanation by Dr Edward Leatham, Consultant Cardiologist
The start of a series of simple video explanations covering all of the main common medical conditions that can affect us, as we age.
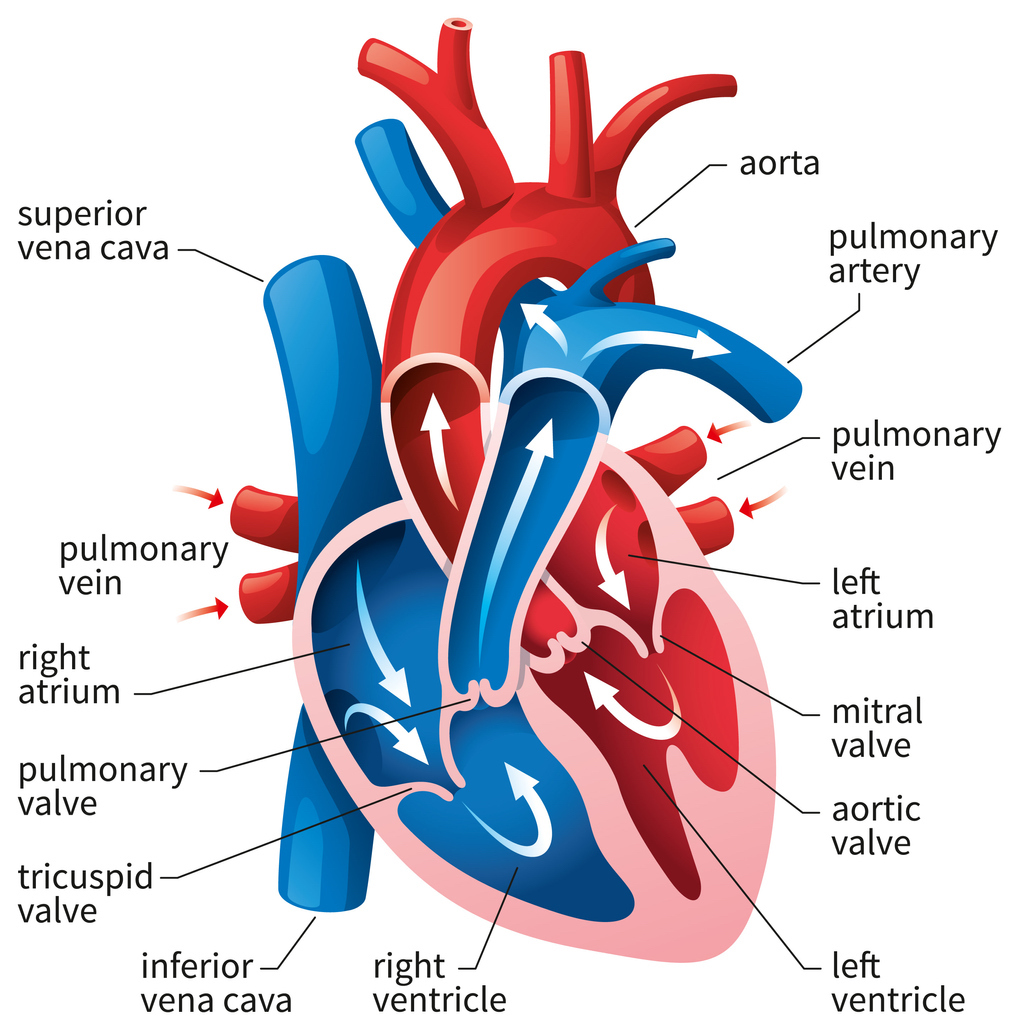
Blood pools in the veins and then returns to the right atrium (which acts like the sump of a petrol engine). This unoxygenated blood is then passed into the right ventricle and pumped into the lungs. There, it is oxygenated by passing through the alveolar capillary bed, picking up oxygen. It then gets returned via pulmonary veins, which lead to the left atrium of the heart. At this point, the left atrium, in normal physiology, contracts as part of the normal cardiac cycle, and the blood is squeezed into the left ventricle. Bear in mind that if the atrium is not working properly, for example, if there is atrial fibrillation, then blood still gets drawn into the left ventricle, because the left ventricle sucks blood in, similar to a fire bellows. As you open the bellows, air is sucked in; similarly, the left ventricle sucks blood in. But if the left atrium is working properly, it will also assist by pushing blood, particularly at the end of diastole during the part of the cycle when the heart fills. In normal hearts that are not stiff, most of the blood drops into the left ventricle without the help of left atrial contraction. As the heart ages or stiffens, the atrial component—the kick caused by atrial systole—becomes increasingly responsible for, or more important for sufficient movement of blood into the left ventricle to empty the pulmonary veins. Just a few tens of milliseconds after the blood enters the left ventricle, the ventricle contracts, the valves connecting the atria and ventricle then close, the valves connecting the ventricle and the rest of the body open—the aortic valve—and oxygenated blood, under the force of contraction of the muscle shortening, exits the left ventricle and circulates around the body. Importantly, just at that moment, 5% of every heart beat passes into the coronary arteries during the next cycle of diastole.
This cycle of filling and contraction in sequence is important for maintaining a wide range of cardiac outputs.