An article written by Dr Edward Leatham, Consultant Cardiologist © 2024 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
Why apply the swiss cheese theory of accident prevention to heart attacks?
Since my research on ‘coronary thrombosis’ in 1996 and 25 years as an interventional cardiologist, I’ve pondered why heart attacks occur unpredictably across individuals with varying levels of coronary plaque and risk factors. The answer seems to lie in the role of chance in heart disease, akin to accidents that result from a series of underlying causes, not just isolated incidents.
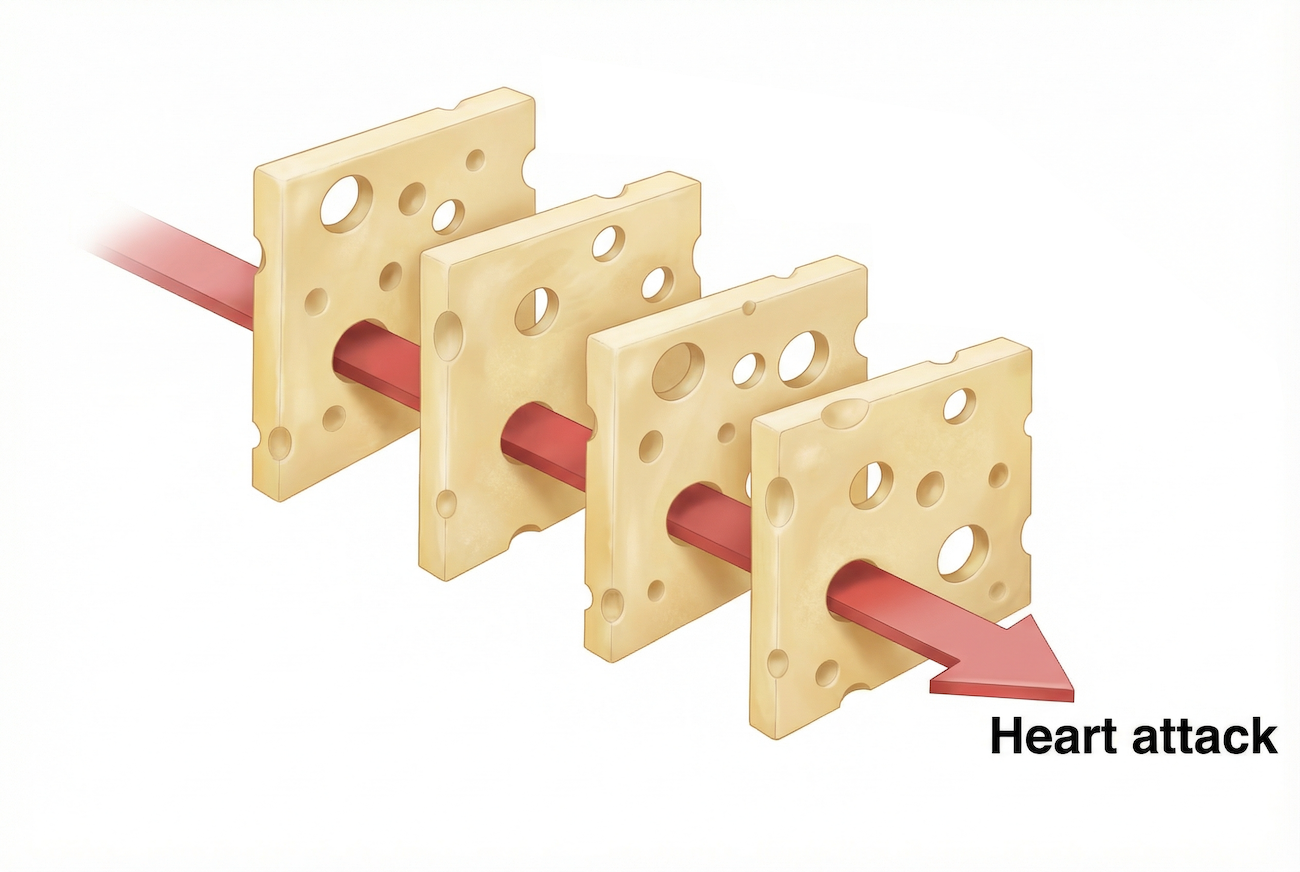
This concept is well illustrated by the Swiss Cheese Model of system accidents. The model describes a stack of spinning disks, each representing a layer of defence with holes. An accident, like a heart attack, occurs when these holes align, allowing hazards to reach victims. In heart disease, the ‘layers’ are biological processes affecting the coronary arteries. A heart attack happens when the ‘holes’ in at least four layers align by chance. Understanding this model helps us realise that heart attack prevention involves more than dealing with just one factor, such as by taking a statin.

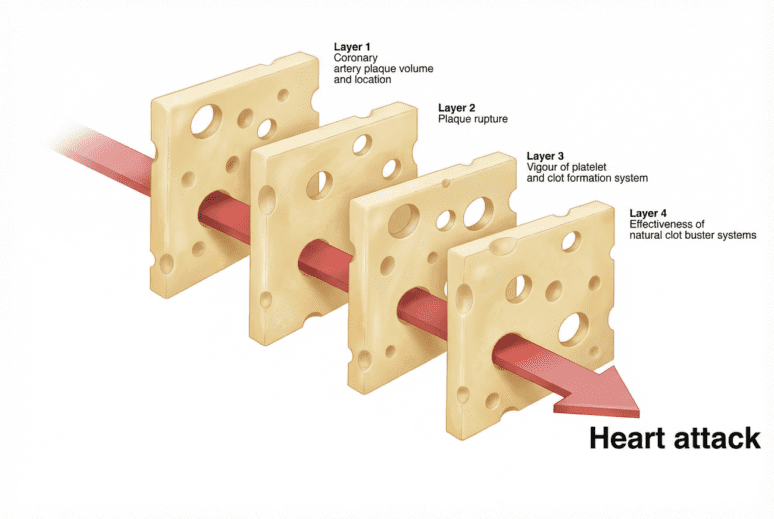
Fig 1. Four identifiable ‘risk’ layers contribute to a heart attack in an individual patient, where the risk of a heart attack can be linked to the number and size of the holes in each layer. Whereas the holes in the first layer can change over many years those in the latter layers vary day by day and even hour by hour. The four layers are spinning and the holes in three of the four distinct layers constantly vary in size as they open and shut thus only align infrequently by chance, explaining the random timing of a heart attack as well as why one patient, even left untreated can have their second event decades after their first.
i. Coronary Plaque
High LDL cholesterol is a principle risk factor for heart disease. Coronary artery disease (CAD) builds up layer by layer, starting in our 20s with fatty streaks in the arteries. Over years, LDL cholesterol laden plaque accumulates, scars and calcificies. The first layer in the Swiss cheese model is therefore the accumulation this soft plaque in and around the coronary arteries, creating the potential for a future heart attack. The risk of a heart attack reduces as the plaque hardens and then calcifies.
ii. The Thin Line between Stability and Disaster
As coronary plaque builds up, it becomes vulnerable to plaque rupture. Plaque vulnerability can lead to temporary thinning of its fibrous cap, increasing the risk of rupture. Inflammatory processes, driven by factors such as raised visceral adipose tissue (VAT), infections, autoimmune diseases, glucose dysregulation and diabetes probably all increase plaque instability. Sudden changes in blood pressure can trigger shear stress on a weakened fibrous cap, causing it to rupture. This concept helps explain why cardiac events are associated with unaccustomed physical exertion.
iii. Thrombosis and Platelets: The Silent Guardians
When plaque ruptures, platelets form a plug to seal off the area, protecting against larger thrombotic proteins. However, the effectiveness of this response varies. During periods of high platelet activation, even minor plaque ruptures can trigger a more aggressive platelet response, leading to clot formation. Antiplatelet drugs like aspirin reduce this risk.
iv. Body’s Fibrinolytic Defence: Our Natural Clot Busters
Our arteries have a clot-busting pathway, the fibrinolytic pathway, which is finely balanced to deal with arterial thrombosis. One of the main regulators of our own fibrinolytic systems is plasminogen activator inhibitor 1 or PAI-1. Factors like statin therapy and exercise improve our ability to handle arterial thrombosis, whereas a sedentary lifestyle and diabetes increase the risk, by increased PAI-1.
Preventive Measures
Understanding heart attacks through the Swiss Cheese Model emphasises the need for a multifaceted approach to prevention. This includes focusing on LDL cholesterol-lowering, good glucose regulation, inhibiting platelets, encouraging exercise, and considering beta-blockers in high-risk patients.
Conclusion
The Swiss Cheese Model provides insight into how multiple factors, when aligned, can lead to catastrophic events like heart attacks. By identifying and reducing these risks through education, intervention, and awareness, we can work towards preventing such tragedies.
Key messages
- When it comes to coronary heart disease, LDL Cholesterol levels are considered to be the main determinant of the build up in coronary plaque. According to this model the ‘risk’ of future heart attack starts with the 1st slice of swiss cheese, the less the plaque, the smaller the holes, the lower the risk.
- If the holes in layers 2, 3 and 4 are small, the risk of heart attack remains low, even with high LDL and plaque, conversely people who have moderate LDL levels and coronary plaque can have transiently large holes appear in layers 2,3 and 4, and when these all line up, this creates the perfect storm for having a heart attack
- By understanding the 4 slices of modifiable risk, and working to reduce hole size in each later the overall risk of future heart attack is lowered far more than by working on one of the layers on its own- so for example taking statins is not as effective as taking statins, regulating glucose and taking regular aerobic exercise.
For other stories related to cholesterol, coronary heart disease, and LDL, explore the archives by entering a tag under the search function above.
Other related articles
- Reason J. Human error: models and management. BMJ. 2000;320:768–70. doi: 10.1136/bmj.320.7237.768. [PubMed]
- Subclinical Coronary Atherosclerosis and Risk for Myocardial Infarction in a Danish Cohort https://www.acpjournals.org/doi/10.7326/M22-3027
- Cardiovascular computed tomography imaging for coronary artery disease risk: plaque, flow and fat: Keith M Channon, David E Newby, Edward D Nicol, John Deanfield http://dx.doi.org/10.1136/heartjnl-2021-320265
- Does Exercise Influence the Susceptibility to Arterial Thrombosis? An Integrative Perspective https://www.frontiersin.org/articles/10.3389/fphys.2021.636027/full
- The Acute and Chronic Effects of Resistance and Aerobic Exercise in Hemostatic Balance: A Brief Review https://www.mdpi.com/2075-4663/11/4/74
The Naked Heart is an educational project owned and operated by Dr Edward Leatham. It comprises a series of blog articles, videos and reels distributed on Tiktok, Youtube and Instagram aimed to help educate both patients and healthcare professionals about cardiology related issues.
If you would like to receive email notification each week from the Naked Heart, follow me on social media or please feel free to subscribe to the Naked Heart email notifications here
FAQ: Understanding Subclinical Coronary Atherosclerosis
1. What is subclinical coronary atherosclerosis?
Subclinical coronary atherosclerosis refers to the build-up of plaque in the coronary arteries, even in the absence of any noticeable symptoms. This plaque build-up, a hallmark of coronary artery disease, often goes undetected until a significant cardiac event occurs.
2. How common is subclinical coronary atherosclerosis?
Studies show that subclinical coronary atherosclerosis is surprisingly common. Research indicates that over 40% of individuals aged 50 to 64 without prior heart issues exhibit some degree of plaque build-up in their arteries. This prevalence increases with age and is more common in men.
3. Can subclinical coronary atherosclerosis lead to a heart attack?
Yes, subclinical coronary atherosclerosis significantly increases the risk of a heart attack. Studies indicate that individuals with obstructive atherosclerosis, even without symptoms, face a notably elevated risk, often exceeding an 8-fold increase compared to those without plaque build-up.
4. What is the relationship between coronary artery calcification (CAC) and subclinical coronary atherosclerosis?
CAC scoring, a measure of calcium deposits in artery walls, often acts as an indicator of plaque build-up. While generally, a higher CAC score correlates with a higher prevalence of atherosclerosis, there are instances where individuals with low or even zero CAC scores show signs of plaque on coronary CT angiography (CCTA).
5. How does the “Swiss Cheese” model explain the occurrence of heart attacks?
The “Swiss Cheese” model illustrates how heart attacks occur despite preventative measures. Each layer of “cheese” represents a safeguard (medication, lifestyle choices, etc.) with potential holes (ineffectiveness, inconsistency). When these holes align, even a minor event like plaque rupture can cascade into a heart attack.
6. How do platelets contribute to heart attack risk in the context of atherosclerosis?
Activated platelets, crucial for blood clotting, play a significant role in atherosclerosis. Upon plaque rupture, activated platelets aggressively clump at the site, potentially forming a dangerous blockage and increasing the risk of a heart attack. Medications like aspirin help mitigate this risk by reducing platelet stickiness.
7. How does the body naturally combat arterial thrombosis (blood clotting)?
The body has a natural clot-busting system known as the fibrinolytic pathway. This system constantly balances clot formation and dissolution to maintain healthy blood flow. Lifestyle choices like regular exercise and medications like statins can improve the efficiency of this system, while factors like a sedentary lifestyle and diabetes can hinder its function.
8. What are the latest guidelines for managing LDL cholesterol to prevent heart attacks?
Recent studies suggest that “lower is better” when it comes to LDL cholesterol levels, particularly for individuals with existing heart conditions or those at high risk. This means there is no established lower limit, and maintaining lower LDL levels with medication can lead to better outcomes.