An article by Dr Edward Leatham, Consultant Cardiologist © 2026 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
In lipid management, percentage LDL reduction is useful, but in cardiology practice it is not enough on its own. The strongest modern position is that clinicians should aim for both a substantial relative reduction in LDL cholesterol and a low absolute LDL level. ESC guidance continues to use this combined approach, with LDL-C goals retained in the 2025 focused update of the 2019 dyslipidaemia guideline. (European Society of Cardiology)
Why does percentage reduction matter? Because trial and meta-analysis data consistently show that cardiovascular risk falls in proportion to the absolute amount of LDL lowered. The Cholesterol Treatment Trialists’ meta-analysis showed about a 22% proportional reduction in major vascular events for each 1 mmol/L LDL-C reduction. (The Lancet)
But percentage reduction alone can mislead. A patient with established coronary heart disease and an LDL-C of 4.5 mmol/L who falls to 2.2 mmol/L on high-intensity statin therapy has achieved roughly a 50% reduction, yet remains above the usual secondary prevention LDL threshold. Biologically, that matters, because arterial wall exposure is driven by particle concentration over time. The practical consequence is simple: a patient can “hit the percentage target” and still remain undertreated.
That is exactly why absolute LDL targets remain essential. In IMPROVE-IT, adding ezetimibe to statin therapy lowered LDL further and improved cardiovascular outcomes. In FOURIER and ODYSSEY OUTCOMES, PCSK9 inhibition pushed LDL down further still and reduced events again. CLEAR Outcomes then extended outcome evidence to bempedoic acid in statin-intolerant patients. Taken together, these trials support a stepwise message: lower is better, and achieving a large percentage fall does not remove the need to get the absolute LDL low enough. (New England Journal of Medicine)
So how should we think about this in clinic?
Percentage reduction tells us whether treatment intensity has been adequate. Absolute LDL tells us whether residual atherogenic risk remains acceptable. One reflects treatment response; the other reflects biological exposure.
For SCVC practice, the most clinically useful formulation is this:
Relative reduction measures how well we have treated. Absolute LDL measures how safe the patient is.
A patient with coronary disease whose LDL falls from 4.5 to 2.2 mmol/L has responded well to treatment, but has not reached a sufficiently low LDL level. That patient usually still needs escalation, typically with ezetimibe first, then PCSK9-targeted therapy where appropriate. This is why the right framework is not absolute versus relative. It is both. (European Society of Cardiology)
Why Non-Pharmacological Strategies Still Matter: Not Alternative, But Additive
In lipid management, there can be a tendency to frame lifestyle and pharmacological therapies as competing approaches. In reality, they operate on complementary biological pathways and are most effective when used together.
Non-pharmacological strategies have three key roles in practice:
- Primary prevention — where lifetime exposure to atherogenic particles can be meaningfully reduced early
- Alternative pathways — in patients who are unwilling, intolerant, or unable to access lipid-lowering medication
- Adjunctive therapy — where they act synergistically with pharmacological treatment to further reduce residual risk
The most important point is that these strategies do not simply produce small incremental benefits. They often target mechanisms that drugs do not fully address, particularly hepatic lipoprotein production, insulin resistance, and visceral adiposity.
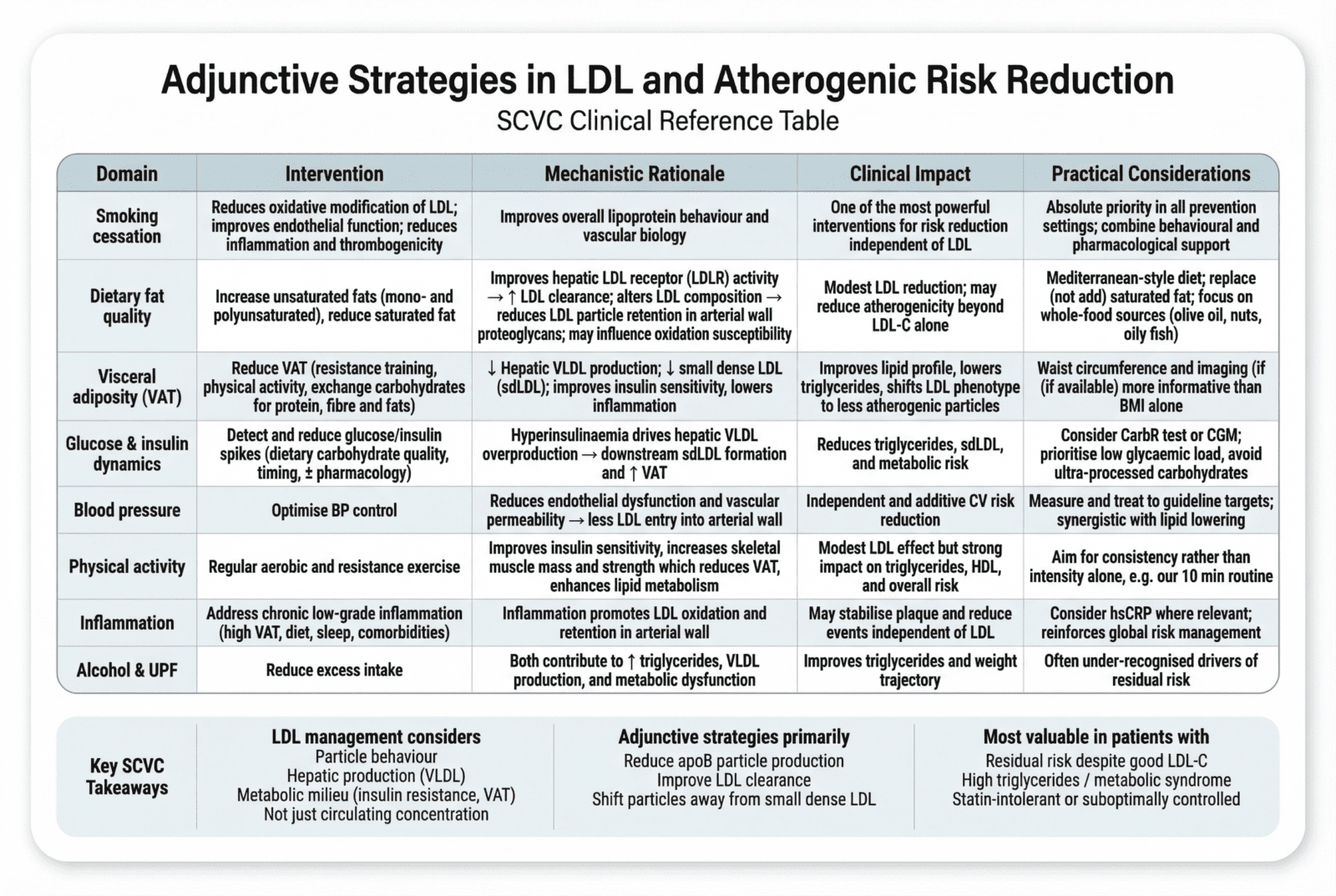
Key Adjunctive Strategies

Mechanistic Rationale for Adjunctive Strategies
While statins and PCSK9-targeted therapies primarily enhance LDL receptor–mediated clearance, non-pharmacological interventions:
- Reduce hepatic VLDL production
- Improve insulin sensitivity
- Shift LDL particles away from small dense, highly atherogenic forms
- Reduce arterial wall exposure and retention dynamics
This creates a synergistic model, where:
- Drugs reduce circulating LDL concentration
- Lifestyle reduces upstream production and downstream atherogenicity
Why This Matters in Patients Already on Therapy
Even in patients achieving LDL targets on pharmacological therapy, residual cardiovascular risk remains substantial. This is often driven by:
- Elevated apoB particle number despite “acceptable” LDL-C
- Persistent small dense LDL phenotype
- Ongoing VLDL overproduction
- Insulin resistance and visceral adiposity
Adjunctive strategies directly address these drivers.
For example:
- A patient on high-intensity statin + ezetimibe may achieve LDL <1.4 mmol/L
- But if they have high VAT and insulin resistance, they may still have:
- Elevated triglycerides
- Increased sdLDL
- High apoB burden
In this setting, lifestyle intervention is not optional—it is mechanistically necessary.
A Synergistic Treatment Model
The most effective cardiovascular prevention strategy integrates both approaches:
- Pharmacological therapy → maximises LDL clearance
- Lifestyle intervention → reduces production and improves metabolic environment
Together, they:
- Lower LDL further
- Improve particle quality
- Reduce arterial wall exposure
- Address residual risk beyond LDL-C
Final Perspective
Non-pharmacological strategies should not be viewed as secondary or optional. They are:
- Essential in primary prevention
- Necessary in those unable or unwilling to take medication
- Critically important as adjunctive therapy in treated patients
In modern cardiovascular prevention, the question is not whether to use lifestyle or medication.
It is how to combine them effectively.
Optimal care is not achieved by choosing one pathway, but by targeting all mechanisms driving atherosclerosis.
Practical take-home message
In high-risk and very high-risk prevention, do not be reassured by percentage reduction alone. If the absolute LDL remains above target, the artery wall still “sees” too much LDL. Good lipid practice is therefore:
Lower LDL substantially, and lower it enough.
Related Blogs
Targets for LDL-C, ApoB and Small Dense LDL
Key references
CTT Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol. Lancet 2010.
URL: https://www.thelancet.com/article/S0140-6736(10)61350-5/fulltext (The Lancet)
2019 ESC/EAS Guidelines for the management of dyslipidaemias.
URL: https://www.escardio.org/guidelines/clinical-practice-guidelines/all-esc-practice-guidelines/dyslipidaemias-management-of/ (European Society of Cardiology)
2025 Focused Update of the 2019 ESC/EAS Guidelines for dyslipidaemias.
URL: https://www.escardio.org/guidelines/clinical-practice-guidelines/all-esc-practice-guidelines/dyslipidaemias/ (European Society of Cardiology)
IMPROVE-IT. Cannon CP et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. NEJM 2015.
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa1410489 (New England Journal of Medicine)
FOURIER. Sabatine MS et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. NEJM 2017.
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa1615664 (New England Journal of Medicine)
ODYSSEY OUTCOMES. Schwartz GG et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. NEJM 2018.
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa1801174 (New England Journal of Medicine)
CLEAR Outcomes. Nissen SE et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. NEJM 2023.
URL: https://www.nejm.org/doi/full/10.1056/NEJMoa2215024 (New England Journal of Medicine)