This article was written by Dr Edward Leatham, Consultant Cardiologist © 2026 E.Leatham. It is an abbreviated version of a chapter from VAT-TRAP: The GLP-1 Advantage.
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available as a story beneath.
If you have been diagnosed with coronary heart disease or high blood pressure, and carry excess weight — especially around your middle — you are not alone. Due to the interaction between our genes, modern lifestyles and diet, visceral fat deposition has become an almost universal feature of ageing. In addition, many people affected also show signs of glucose dysregulation — often referred to as non-diabetic hyperglycaemia — which is associated with insulin resistance. Together, these factors can significantly affect your healthspan.
The current accepted medical practice is to reserve modern medicines and treat once someone develop diabetes. However it can be argued that the key should be to prevent non diabetic hyperglycaemia state developing into full blown diabetes, which is often associated with multiple complications. Metabolic dysfunction -associated steatotic liver disease MASLD, also known as fatty liver/NAFLD-non alcoholic liver disease, is a condition commonly associated with being overweight. Fatty changes are seen within the liver which could lead to chronic liver disease. In both non diabetic hyperglycaemia and MASLD, the focus should be reversing the glucose dysregulation and reducing visceral fat at the onset rather than waiting for the complications to develop.
These conditions often occur together and are linked by a common underlying issue: metabolic dysfunction. The encouraging news is that we now understand this process can often be slowed — and in many cases, even reversed. Better still, we are learning to do this more effectively through a powerful combination of modern medication, technology, and lifestyle change.
In this blog, I will introduce an approach we started at my clinic in 2025 referred to as the Metabolic Reset — a structured 8-month programme that uses modern tools such as GLP-1 mimetic injections, continuous glucose monitoring (CGM), a food analysis app, resistance training, and a protein-forward diet. The aim is to reduce visceral fat, build muscle strength, and reboot your metabolism — with the ultimate goal of minimising the need for long-term medication.
It is worth noting that, prior to joining the programme, many of our patients undergo a metabolic health assessment wearing a CGM and keeping a detailed food diary. This helps us assess the degree of glucose dysregulation and carbohydrate sensitivity present. In milder cases of non-diabetic hyperglycaemia, patients can use our toolkit to address these issues without the need for GLP-1 mimetic therapy — with the option to escalate to a pharmacologically assisted Metabolic Reset, only if needed.
Why Target Visceral Fat and Muscle Mass/Strength?
Two key, modifiable drivers of poor metabolic health are:
- Visceral fat: This is the harmful fat stored deep in the abdomen around your organs. It is strongly linked to high blood pressure, fatty liver, insulin resistance, and cardiovascular disease.
- Skeletal muscle mass and strength: Muscle is the engine of your metabolism. It helps burn glucose, regulate insulin, and support a healthy weight.
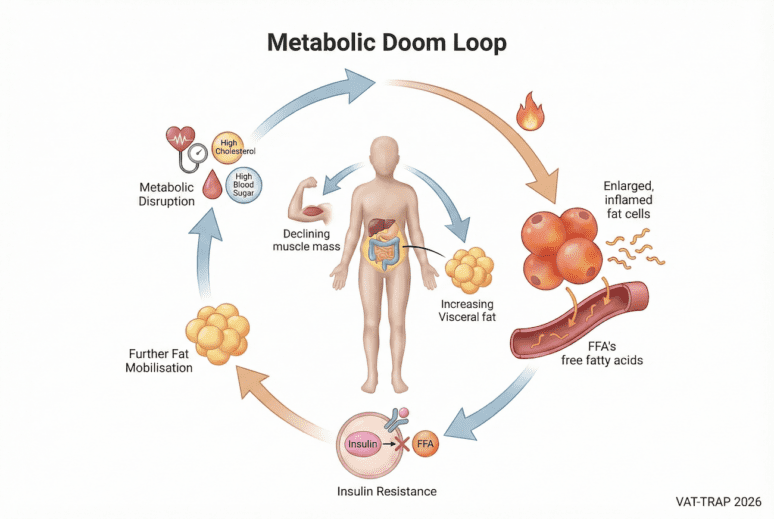
As we age, our body composition gradually changes. Because of anabolic resistance ( a topic covered in another blog) both muscle mass and strength decline from 30 years of age, while visceral fat — the fat stored around internal organs — tends to increase. Many people also carry a genetic predisposition that makes them more vulnerable to metabolic problems when exposed to modern diets and sedentary lifestyles. Over time, this combination drives higher blood pressure, rising cholesterol and triglycerides, and worsening blood sugar control — the cluster of problems known as metabolic syndrome.
Visceral fat is not just passive storage; it is metabolically active and inflammatory. As fat cells enlarge and become overfilled, they begin releasing free fatty acids (FFAs) into circulation. These FFAs interfere with insulin signalling in muscle and liver tissue, reducing the body’s ability to process glucose efficiently. This can create a self-reinforcing cycle — sometimes described as a “metabolic doom loop” — where insulin resistance leads to further fat mobilisation and ongoing metabolic disruption.

The encouraging news is that this process is often reversible. Reducing visceral fat, rebuilding skeletal muscle, and creating a sustainable energy deficit can improve insulin sensitivity and restore metabolic health.
Introducing the 8-Month Metabolic Reset Programme
This reset is not a fad diet or quick fix. It is a structured intervention we use in our cardiometabolic clinic designed to change your body from the inside out, addressing the root causes of your metabolic problems. Here is what it involves:
1. Continuous Glucose Monitoring (CGM): Personalised Nutritional Feedback
Continuous glucose monitoring (CGM) provides real-time insight into how blood glucose responds to food, activity, stress, and sleep. Many people are unaware of how differently their bodies respond to specific meals until they see these patterns displayed continuously. A small wearable sensor measures interstitial glucose throughout the day, allowing personalised feedback rather than relying solely on occasional blood tests.
Glucose excursions after meals are common, even in individuals without diabetes. However, larger or more prolonged postprandial glucose rises may reflect reduced metabolic flexibility and early insulin resistance, where skeletal muscle and liver are less able to efficiently clear incoming glucose. In response, insulin secretion increases to facilitate glucose storage and suppress hepatic glucose output. When energy intake persistently exceeds immediate requirements, the liver can convert excess carbohydrate into fatty acids and triglycerides, which are exported as very-low-density lipoprotein (VLDL) particles and stored within adipose tissue.
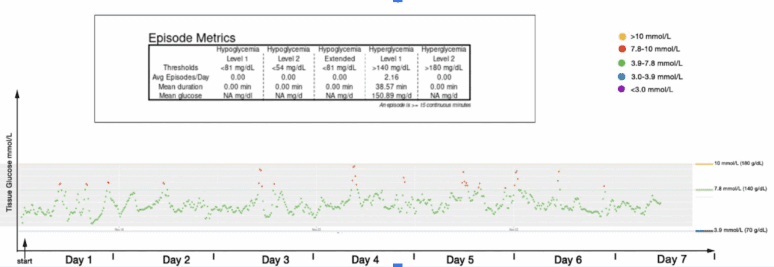
In some non-diabetic individuals with normal HbA1c levels, CGM may still reveal periodic glucose excursions above 7.8 mmol/L after carbohydrate-rich meals — a pattern that is not uncommon and may indicate early metabolic stress rather than overt disease.
In this non -diabetic patient with a normal HbA1c, there are an average of 2 glucose excursions of blood glucose > 7.8 mmol/L per day related to carbohydrate intake, a pattern seen in many similar patients.
For individuals with prediabetes or early glucose dysregulation, CGM can be a powerful educational tool. It helps patients to:
- Identify foods and eating patterns that produce large glucose excursions
- Select lower-glycaemic or less processed alternatives that promote glucose stability
- Observe improvements in postprandial glucose control as visceral fat decreases and insulin sensitivity improves
In this programme, CGM serves as both a learning tool and a motivator, empowering you to take control of your food choices with immediate feedback. Our clinic also operates direct access CGM testing with a professional report.
2. Protein-Forward Diet: Fuel Muscle and Satiety
As visceral fat is reduced, it is vital to protect and build muscle mass and strength — particularly for individuals over the age of 50. This requires two key elements:
- Adequate protein intake — to provide the amino acids needed for muscle repair and maintenance
- Resistance training — to signal the body to preserve or increase muscle mass
Most people do not consume sufficient protein for metabolic health. In this programme, we aim for:
- 1.2–1.6 grams of protein per kilogram of body weight per day
- Protein at each meal, not just in the evening
- Meals paired with fibre-rich vegetables and healthy fats
Importantly, protein also stimulates your own natural GLP-1 production. That means that over time, your body begins to regulate appetite more effectively — helping you transition off medication.
3. Resistance Training: Rebuild the Metabolic Engine
Muscle does more than move the body — it acts as a metabolic powerhouse. Stronger muscle means better insulin sensitivity, improved glucose control, and greater calorie expenditure at rest.
Even basic resistance training (2–3 times per week) can:
- Lower blood glucose
- Improve insulin resistance
- Increase resting metabolic rate
- Prevent age-related muscle loss (sarcopenia)
You do not need to join a gym. Simple home-based exercises using body weight, resistance bands, or light dumbbells are a great place to begin. The priority is consistency and progression. We recommend a 10 minute routine at home 5 – 7 days a week as a basic, longterm lifestyle change.
4. GLP-1 Mimetics: Kickstarting Fat Loss and Appetite Reset
GLP-1 mimetics are a class of medications, typically administered as once-weekly injections, that replicate the action of the naturally occurring hormone glucagon-like peptide-1 (GLP-1). These medications:
- Suppress appetite
- Slow gastric emptying
- Enhance glucose-dependent insulin release after meals
- Reduce glucagon secretion (which otherwise raises blood glucose)
- Support weight loss, particularly reduction in visceral adiposity
- Break the metabolic doom loop
For patients with cardiovascular disease or glucose dysregulation, GLP-1–based therapies can offer both metabolic and cardiovascular benefit when used appropriately within a supervised clinical framework.
Within this programme, GLP-1 mimetics are used for a defined period — typically around eight months — alongside sustainable dietary and lifestyle change. Treatment often starts at low (even micro) doses, with gradual dose escalation according to tolerance and clinical response. Importantly, the goal is not indefinite pharmacological weight management. Instead, these agents are used strategically to help reduce visceral fat at the centre of the metabolic “doom loop,” support metabolic resetting, and create a physiological and behavioural springboard for lasting lifestyle change.
What to Expect Over 8 Months
Month 1–2: Initiation Phase
- Agree on target achievable weight and waist at the beginning. If you have access to a DEXA/CT/MRI measurement of your visceral adipose tissue score, this helps define a metabolically healthy waist target.
- Introduce basic resistance training
- Transition diet: increase protein, reduce refined carbohydrates
- Start GLP-1 mimetic at low dose, increase as tolerated and required for slow but steady progress – like with all dietary programs, lowering a defended weight /adipose set point need to be done slowly.
- Consider using CGM to assess glycaemic response to foods (especially if you were glucose dysregulated before)
Expected outcomes: Appetite reduction, 2–5% waist circumference and weight loss, early visceral fat reduction, improved post-meal glucose responses
Month 3–5: Acceleration Phase
- Reach therapeutic steady GLP-1 dose
- Use CGM data to guide food choices where necessary
- Resistance training becomes part of routine and needs to be progressive (ie once strength improves and it becomes easy, lift heavier weights)
- Waist circumference continues to drop, even if weight remains steady (as muscle weighs more than adipose tissue)
- Likely improvement in glycaemic and MASLD blood markers
Expected outcomes: 5–10% total body weight loss, increased insulin sensitivity, improved energy levels, lowered blood pressure
Month 6–8: Transition Phase
- Emphasis shifts to muscle preservation and metabolic independence
- Protein intake and strength training remain central
- For those reaching waist goals, begin tapering GLP-1 dose under supervision
Expected outcomes: Stable lean mass, reduced visceral fat, better metabolic flexibility, readiness to stop medication
How Do We Measure Success?
This programme looks beyond the bathroom scales. We track:
- Waist circumference — a practical marker of visceral fat loss
- Functional improvements — such as heaviest weight that can be lifted on outstretched arms, walking stamina, stair times
- Food group quantification – using Dr Shape, an AI-guidied food analysis app
- Medical-grade strength measurements – handgrip meter for upper and sit to stand testing for lower muscle strength see blog
- Blood pressure and HbA1c — for cardiovascular and metabolic risk reduction
There are also options to also track:
Body composition — low dose VAT CT or DEXA scans. Smart scales can provide useful additional data as long as taken in context (GLP-1 mimetics alter muscle glycogen that can disrupt body composition readings).
CGM trends — with fewer glucose spikes after meals.
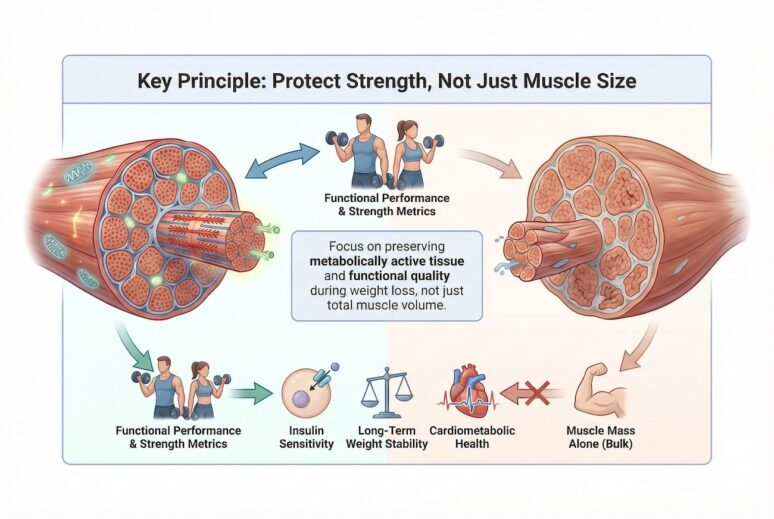
It is important to note that for older patients, tracking muscle volume may be misleading and can be a poor indicator of good progress, which is why strength, linked to metabolic function is a better metric to track.
Is This Just Another Weight-Loss Programme?
No — this is not a “slimming club” or crash diet.
The Metabolic Reset is a clinically designed, time-limited intervention aimed at reversing the biological causes of weight gain, glucose problems, and high blood pressure. By reshaping body composition and restoring metabolic balance, we are not just treating symptoms — we are tackling the root cause.
Can I Stop the Injections After 8 Months?
In many cases, yes — that is the intended goal.
If, by the end of the programme, you have:
- Reduced visceral fat to a metabolically healthier level, helping to break the metabolic “doom loop”
- Increased or preserved skeletal muscle strength
- Achieved stable post-meal glucose patterns on CGM
- Established sustainable nutrition and physical activity habits
…then it may be appropriate to gradually taper off GLP-1 mimetics with minimal rebound weight gain or deterioration in metabolic markers. Any dose reduction or discontinuation is undertaken under medical supervision, with a personalised plan agreed at the end of the programme.
This plan may include ongoing monitoring and, in some cases, intermittent low-dose GLP-1 use triggered by early warning signs of metabolic drift — for example, increasing waist circumference or rising glucose variability.
The key principle is that medication acts as a bridge, not the destination. The aim is to use pharmacological support to create metabolic momentum while long-term habits, muscle preservation, and lifestyle change become the primary drivers of continued success.
There may be periods — such as winter months or festive seasons — when metabolic control becomes more challenging despite best efforts. In selected cases, short-term reintroduction of low-dose GLP-1 support may be considered as part of a structured long-term strategy rather than continuous treatment. For example , over wintertime feasting months when metabolic health can slip despite our best efforts, there may be a need for some temporary return to GLP-1 support. We all know “Dry January”; some patients jokingly refer to a short metabolic reset period as “Jab January.”
Final Thoughts:
Every week I meet patients who feel stuck — in a cycle of weight gain, fatigue, medication, and worsening blood pressure or blood sugar. But your body is capable of change. With the right tools, knowledge, and support, you can rebuild a healthier metabolism.
If you have cardiovascular disease, carry excess weight, or have signs of insulin resistance, you do not need to wait until diabetes develops. This structured reset can change your trajectory.
It is not easy — but it is achievable. And it is worth it.
Interested in a Reset?
Speak to your doctor or see our GLP-1 mimetic clinic to discuss:
- Whether GLP-1 mimetics are appropriate for you
- Using a CGM to understand your unique glucose responses
- Support for nutrition and resistance training tailored to your needs
We are no longer just managing numbers. We are restoring metabolic health from the inside out.
Related posts and articles
- Why Protein Matters More Than Ever as We Age
- Sarcopenia: Are We Diagnosing the Correct Muscle Problem?
- Protein, Sarcopenia, and the Pursuit of Healthspan
- Visceral adipose tissue and residual cardiovascular risk: a pathological link and new therapeutic options 2023
- How to Lose Visceral Adipose Tissue (VAT) and Improve Metabolic Health: A Guide to Sustainable Weight Loss
- Dietary Fats: From Villain to Vital Nutrient – Rethinking Fat in a Heart-Healthy Diet
- Protein, Sarcopenia, and the Pursuit of Healthspan