Dr Edward Leatham, Consultant Cardiologist
© 2024 E. Leatham
Continuous glucose monitors (CGMs) that do not require regular finger-prick calibration only became widely available in 2016.[1] These devices were developed primarily to help insulin-dependent patients with diabetes detect and prevent hypoglycaemic episodes—serious events that continue to cause substantial morbidity, hospitalisation, and mortality worldwide.
By measuring glucose levels in interstitial fluid throughout the day, CGMs provide near real-time insight into glucose patterns. This allows patients and clinicians to identify dangerous lows, reduce glucose variability, and increase the amount of time spent within the recommended glucose range (“time in range”).
Clinical trials have confirmed that CGMs improve glycaemic control and safety in diabetes care, representing one of the most important technological advances in diabetes management in recent decades.
However, their potential use may extend far beyond diabetes.
Glucose Spikes in People Without Diabetes
Around 2018, researchers began exploring CGM use in individuals without diabetes. Early observational studies and reports produced a surprising finding: many apparently healthy individuals experience significant spikes in glucose levels after meals.
These post-meal rises can occasionally reach levels that would traditionally be associated with impaired glucose metabolism.
Importantly, individuals with these responses often do not meet the diagnostic criteria for pre-diabetes or Type 2 diabetes. Yet their glucose patterns may fluctuate considerably depending on the foods they consume.
Unlike hypoglycaemia, elevated glucose levels rarely cause immediate symptoms. In this respect they resemble high blood pressure—silent in the short term but potentially important over time. Low glucose levels, however, may trigger symptoms such as fatigue, hunger, or irritability, which can drive further snacking and reinforce unhealthy dietary habits.
These observations have led to growing interest in the concepts of glucose dysregulation and glucose variability, both of which are now being investigated as potential contributors to long-term disease.
Why Glucose Variability Might Matter
Chronic diseases such as coronary artery disease, dementia, and inflammatory conditions develop over many years. While traditional risk factors such as cholesterol, smoking, and blood pressure remain critically important, they do not fully explain why some individuals develop disease while others do not.
In patients with diabetes, poor glucose control is known to accelerate atherosclerosis and worsen cardiovascular outcomes. Higher glucose variability has been associated with worse outcomes following acute coronary syndromes and higher rates of restenosis after coronary stenting.
Large population studies have also shown that simple measures of glucose variability are associated with increased future cardiovascular risk.
Whether similar mechanisms operate in individuals without diabetes is currently unknown. The necessary prospective studies simply have not yet been conducted. Nevertheless, the hypothesis that glucose variability may contribute to vascular inflammation and cardiovascular risk is biologically plausible and increasingly discussed within metabolic and cardiovascular research.
The Growing Popularity of CGMs
Interest in CGMs has grown rapidly outside the traditional diabetes population. Consumer health platforms such as Zoe have popularised the idea that monitoring individual responses to food can help guide personalised nutrition.
As a result, CGMs are becoming increasingly accessible and are now widely available online and through pharmacies. A rapidly expanding commercial market has emerged around glucose monitoring for “metabolic optimisation”.
While this enthusiasm reflects genuine interest in metabolic health, it also highlights the need for careful interpretation of the data these devices provide.
A Note of Medical Caution
Medicine has repeatedly shown that plausible theories do not always translate into improved clinical outcomes.
One of the most striking examples is the ACCORD trial, published in the New England Journal of Medicine in 2008.[2,3] The study examined whether aggressive glucose lowering in patients with Type 2 diabetes would reduce cardiovascular events. Unexpectedly, the intensive treatment arm showed higher mortality, leading to early termination of the trial.
Similarly, epidemiological studies have shown that while high HbA1c levels are associated with increased cardiovascular risk, very low HbA1c levels may also be associated with increased all-cause mortality in some populations.[4]
These observations remind us that metabolic systems are complex, and interventions that appear logical must always be tested carefully in well-designed trials.
A Pragmatic Approach in Clinical Practice
Despite the current lack of definitive evidence, CGMs can still provide useful insights when interpreted thoughtfully.
When reviewing CGM traces in clinical practice, clear differences are often seen between individuals with stable metabolic responses and those with large post-meal glucose excursions.
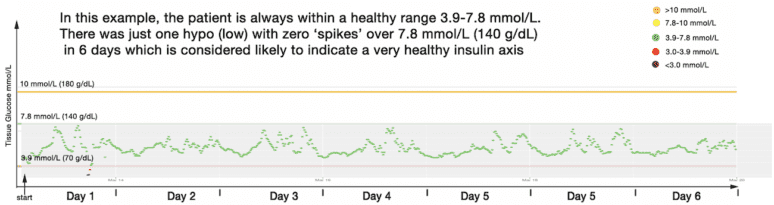
Fig 1

CGM trace from a metabolically healthy individual showing stable glucose levels predominantly within the 3.9–7.8 mmol/L range, with minimal post-meal excursions.
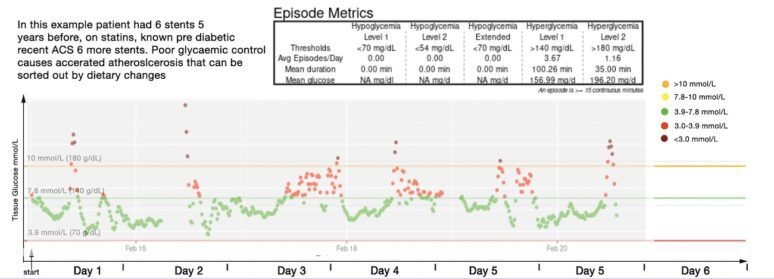
Fig 2
CGM trace from a patient with progressive coronary artery disease despite low LDL levels, demonstrating repeated post-meal glucose excursions above 7.8 mmol/L.
In situations such as the example shown in Fig 2, it seems reasonable to encourage patients to aim for post-meal glucose levels below approximately 7.8 mmol/L (140 mg/dL) where feasible.
This is not presented as proven therapy, but rather as a practical lifestyle target that aligns with established metabolic health ranges.
Interpreting CGM Data
CGMs are not as precise as laboratory glucose measurements, particularly at very low glucose concentrations (<3 mmol/L). However, they appear sufficiently accurate to demonstrate real-time responses to food intake and daily lifestyle patterns.
In our own analysis of CGM data, we standardise axes on episode-metrics graphs to allow consistent comparison between individuals.
Based on diabetes literature and international consensus standards, we broadly interpret glucose ranges as follows:
Healthy range
- 3.9–7.8 mmol/L (70–140 mg/dL)
Mildly elevated
Clearly elevated
Providing patients with clear visual feedback about their glucose responses can often motivate meaningful lifestyle change.
Lifestyle Changes That Improve Glucose Responses
Several simple strategies appear to reduce post-meal glucose spikes:
- Increasing dietary fibre intake
- Reducing refined carbohydrate consumption
- Prioritising protein and fibre at breakfast
- Improving sleep quality
- Increasing daily physical activity
In many patients, particularly those with high-carbohydrate breakfast habits, modest dietary changes can produce measurable improvements in glucose regulation within a few months.
Emerging research also suggests that these improvements may partly reflect beneficial changes in the gut microbiome.
Importantly, these lifestyle interventions carry minimal risk and may improve overall metabolic health regardless of whether glucose variability proves to be a causal factor in cardiovascular disease.
Pharmacological Intervention: Not Yet Justified
A more controversial idea is the use of glucose-lowering medications in individuals without diabetes who demonstrate glucose dysregulation on CGM.
At present, there is insufficient evidence to support such an approach outside well-designed clinical trials. Until robust outcome data become available, pharmacological treatment in this setting remains difficult to justify.
The emphasis should therefore remain on lifestyle and dietary strategies.
Conclusion
Continuous glucose monitoring has transformed the management of diabetes and is now offering new insights into metabolic health more broadly.
For patients with coronary artery disease who demonstrate large post-meal glucose excursions, modest dietary adjustments aimed at reducing glucose variability may represent a sensible and low-risk strategy.
Even if future research ultimately shows that glucose variability is not a primary driver of disease, the lifestyle improvements encouraged by CGM insights—better diet, weight loss, and increased metabolic awareness—are likely to deliver meaningful health benefits.
The rapid evolution of CGM technology illustrates how advances in monitoring can reshape our understanding of disease and open new avenues for prevention.
References
- Introduction: History of Glucose Monitoring
- ACCORD Trial Effects of Intensive Glucose Lowering in Type 2 Diabetes 2008
- NPC Archive Item: Increased death rate found in intensive blood glucose-lowering arm of trial in type 2 diabetes – study arm halted