An article written by Dr Edward Leatham, Consultant Cardiologist © 2025 E.Leatham
Tags: VAT, GLP-1, Inflammation, Diet, CKD, search website using Tags to find related stories.
In a related article, I explored how your mitochondria — the cellular “power stations” that produce energy — can become overwhelmed by surplus fuel, especially in the form of glucose.
When mitochondria process more fuel than your body needs, they begin to leak free radicals, triggering inflammation and long-term damage.
But under normal circumstances, how does excess energy get managed, when it can’t be immediately used?
It’s stored as fat — and the location of that fat matters far more than most people realise.
Today, we are looking at visceral fat — what it is, why it’s so dangerous, and how it’s part of a vicious metabolic feedback loop involving glucose overload, inflammation, and declining muscle function.
🔍 What Is Visceral Fat (VAT)?
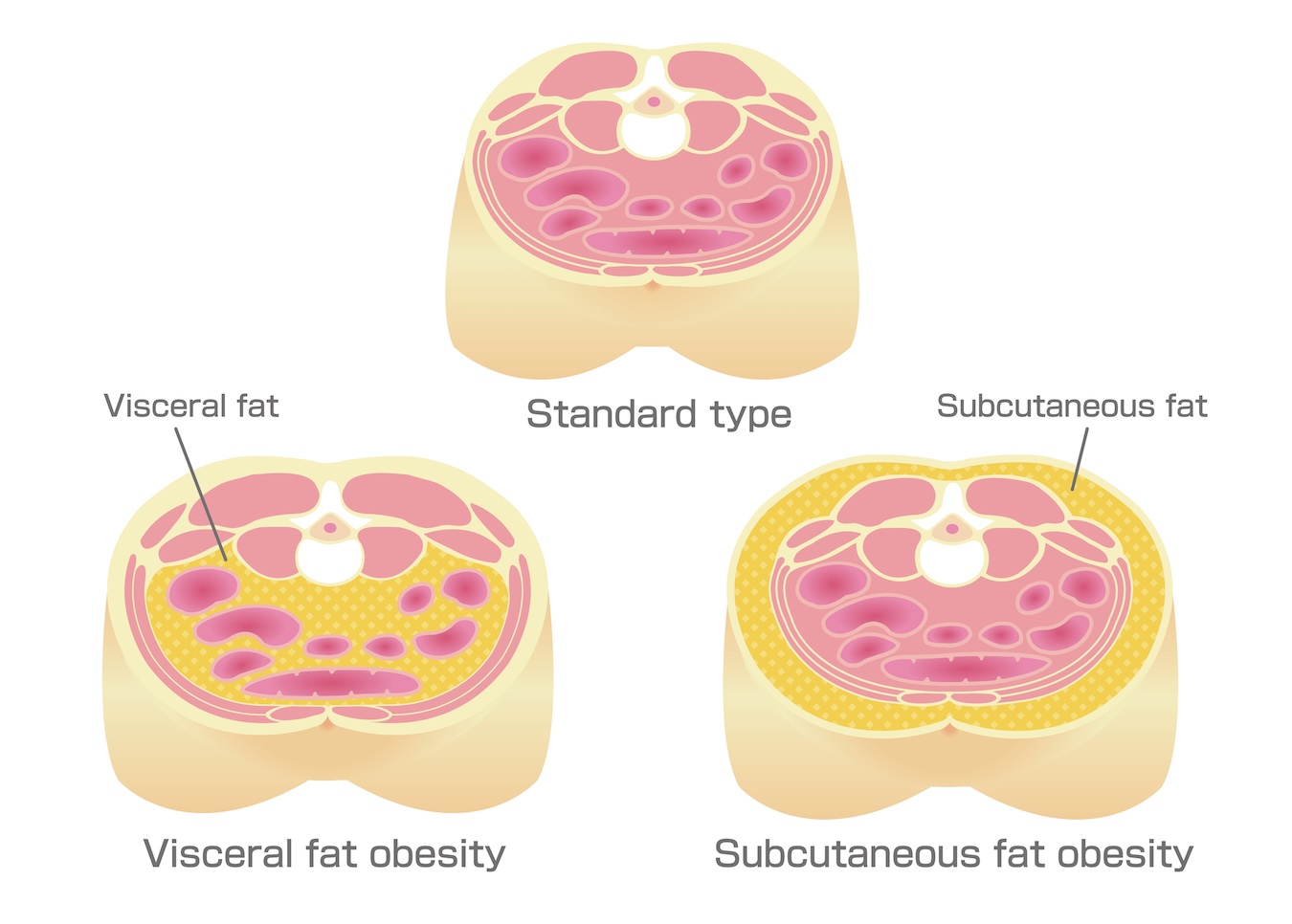
Visceral adipose tissue — or VAT — is the fat stored deep inside your abdomen, wrapped around your organs: liver, intestines, pancreas, kidneys. In small quantities it is protective by cushioning the vital organs
When present in excess, visceral adipose tissue is different from subcutaneous fat (the soft, pinchable kind under your skin). VAT is hidden, but far more metabolically active — and problematic.
VAT acts like a rogue endocrine organ. It doesn’t just store energy. It releases inflammatory molecules, interferes with insulin sensitivity, and is strongly linked to:
- Type 2 diabetes
- Heart disease
- Stroke
- Fatty liver disease
- Cognitive decline
As VAT grows it starts to push your abdomen out and your waist circumference grows. In fact, due to the negative effects of visceral fat, your waist-to-height ratio is now recognised as a more powerful predictor of metabolic risk than BMI.
🍞 From Glucose Spikes to Fat Storage: A Problem of Overflow
Every time you eat a high-carbohydrate meal — especially one low in fibre and protein — your blood glucose rises. If your muscles are active and insulin is functioning well, that glucose is taken up and burned for energy. In people with a carbohydrate sensitive phenotype it appears the glucose clearance systems are not sufficient to clear the surplus so you can see short periods of high glucose in the circulation (spikes) as an early sign of the problem.
However it is clear whether you have csp or not , if your muscle mass is low (as in age-related sarcopenia), or you are sedentary, or your mitochondria are already saturated with fuel, the insulin triggered by the rise in glucose will signal storage processing, initially short term glycogen in muscle and liver then converting to Triglycerides for long term storage (your battery).
As we explained in a related blog on mitochondria, this is like solar panels producing too much energy for a full battery — the system overheats, and damage follows.
In the body, this excess energy is redirected into fat storage.
At first, it accumulates in subcutaneous tissue. But over time — especially in genetically susceptible people — fat begins to collect viscerally, inside the abdominal cavity.
🧬 Some Bodies Store Fat Differently
Not everyone responds the same way to surplus calories — particularly carbohydrates.
- Some people have genetic polymorphisms that impair their ability to safely store or clear glucose.
- Others have a carbohydrate-sensitive phenotype (CSP), meaning even “normal” meals spike their glucose significantly.
- For these individuals, energy overload leads more rapidly to visceral fat accumulation, even when BMI is not especially high.
In clinic, we see patients with “normal” weight but large waist circumferences, significant VAT on CT scans, and signs of early insulin resistance or inflammation — all driven by a mismatch between intake, clearance, and demand.
🔁 The Vicious Cycle: VAT, Muscle, and Mitochondrial Overload
Here’s where things get really dangerous.
As VAT expands, it starts doing much more than storing fat:
- It releases free fatty acids (FFA) into the bloodstream, especially through the portal vein to the liver
- It secretes inflammatory cytokines like TNF-α and IL-6
- It recruits immune cells, increasing tissue inflammation
- It impairs insulin sensitivity in nearby tissues, including skeletal muscle
This creates a vicious cycle:
More VAT → more FFA + inflammation → insulin resistance → reduced glucose disposal by muscle → more glucose in bloodstream → more fat storage (especially visceral)
Meanwhile, ageing reduces muscle mass (sarcopenia), further decreasing the body’s ability to absorb and use glucose efficiently. Mitochondrial function declines, especially in muscle and liver, compounding the problem.
🧪 Why VAT Is So Toxic
VAT is more dangerous than subcutaneous fat because it is:
- Highly vascularised — it dumps FFA directly into the liver
- Hypoxic and inflamed — it accumulates immune cells and produces ROS
- Hormone-active — it releases adipokines that interfere with metabolism
- Harder to lose — it often persists even as total body weight drops
VAT contributes to the development of:
- Fatty liver
- Hypertriglyceridaemia
- Hypertension
- Pro-atherogenic lipid profiles
- Glucose intolerance and type 2 diabetes
And it does so not just by being “extra fat,” but by actively sabotaging mitochondrial and muscle function.
👩⚕️ Breaking the Cycle
To reverse this cycle, we need to:
- Restore muscle mass — resistance training increases glucose uptake and mitochondrial density
- Blunt glucose spikes — CGM, low-glycaemic eating, and fasting can help
- Reduce VAT directly — by creating a modest, consistent energy deficit and increasing fat oxidation
- Reboot mitochondria — using fasting, movement, and mitochondrial-supportive nutrients
- Identify those with CSP — and tailor diets to avoid glycaemic overload in genetically vulnerable patients
The earlier this cycle is identified, the more reversible it is.
🔁 Recap: Mitochondria, Muscle and Visceral Fat
| Factor | Effect |
|---|
| Excess glucose | Overloads mitochondria → ROS → inflammation |
| Ageing + inactivity | Muscle loss → reduced glucose clearance |
| VAT growth | Releases FFA + cytokines → worsens insulin resistance |
| Inflammation | Further impairs mitochondrial function |
| Result | Accelerated metabolic dysfunction and ageing |
📌 Final Thoughts
VAT is not just a by-product of weight gain — it is a key player in metabolic disease.
Its expansion is often the body’s final attempt to store energy that cannot be used or burned. But once it reaches a certain threshold, VAT becomes inflammatory, insulin-resistant, and metabolically toxic.
To prevent this, we must understand how modern life — constant food intake, refined carbohydrates, sedentary routines — overwhelms the mitochondria, depletes muscle, and promotes visceral fat storage.
When you see VAT not just as fat, but as a marker of mitochondrial overload, everything changes.
📚 References
- Ashwell M, Gibson S. Waist-to-height ratio as an indicator of ‘early health risk’. BMJ Open. 2016;6(3):e010159.
https://bmjopen.bmj.com/content/6/3/e010159 - Zeevi D et al. Personalized nutrition by prediction of glycemic responses. Cell. 2015;163(5):1079–94.
https://www.cell.com/cell/fulltext/S0092-8674(15)01481-6 - Kawai T, Autieri MV, Scalia R. Adipose tissue inflammation and metabolic dysfunction. Am J Physiol Cell Physiol. 2021;320(5):C375–C391.
https://journals.physiology.org/doi/abs/10.1152/ajpcell.00379.2020 - Ouchi N, Parker JL, Lugus JJ, Walsh K. Adipokines in inflammation and metabolic disease. Nat Rev Immunol. 2011;11(2):85–97.
https://www.nature.com/articles/nri2921 - Lanza IR, Short DK, et al. Endurance exercise as a means to improve mitochondrial function in aging. J Clin Invest. 2015;125(2):615–23.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4319423/
Other related articles
- Mitochondria: The Tiny Engines Managing Your Energy — Until They Are Overloaded
- Carbohydrate Sensitive Phenotype (CSP): Precursor of the Metabolic Syndrome?
- Anthropometrics vs BMI: Why Waist Measures Outperform BMI in Cardiovascular Risk Assessment
- Why I Eat a Cooked Breakfast to Lower My Visceral Fat
- “Why Am I Out of Breath?” — The Hidden Link Between Belly Fat and Breathlessness
- Why everyone is talking about VAT
- How to Lose Visceral Adipose Tissue (VAT) and Improve Metabolic Health: A Guide to Sustainable Weight Loss
- The Expanding Waistline in Men: Spare Tyre, Killer Visceral Fat, or Just Flabby Abdominal muscles?
- From Genes to Greens: How DNA Shapes Your Nutritional Needs
- The 8-Month Metabolic Reset: A New Approach to Reversing Visceral Fat, Improving Blood Pressure and Blood Glucose