An article by Dr Edward Leatham, Consultant Cardiologist © 2026 E.Leatham
For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath.
The Usual Recommendation
If you are diagnosed with atrial fibrillation (AF) or Atrial flutter (Aflutter), whether it is long term (accepted), atrial fibrillation/flutter, persistent atrial fibrillation/flutter or paroxysmal atrial fibrillation/flutter IF your CHA₂DS₂-VASc score is 2 or higher, current guidelines generally recommend long-term anticoagulation.
👉 You can calculate your CHA₂DS₂-VASc score here:
This is because AF and Aflutter increase the risk of stroke, and anticoagulants significantly reduce that risk.
But What If You’ve Only Had One or infrequent Episode(s)?
A common and very reasonable question is:
“If I’ve only had one episode of paroxysmal atrial fibrillation (PAF), do I really need anticoagulants for life?”
The answer is:
👉 Not always—but it depends on several important factors.
Why Guidelines Recommend Anticoagulation
Even a single documented episode of AF or flutter can be significant because:
- AF and Aflutter may recur without symptoms (silent AF)
- Stroke risk is driven more by underlying risk factors (CHA₂DS₂-VASc) than by AF/Aflutter frequency alone
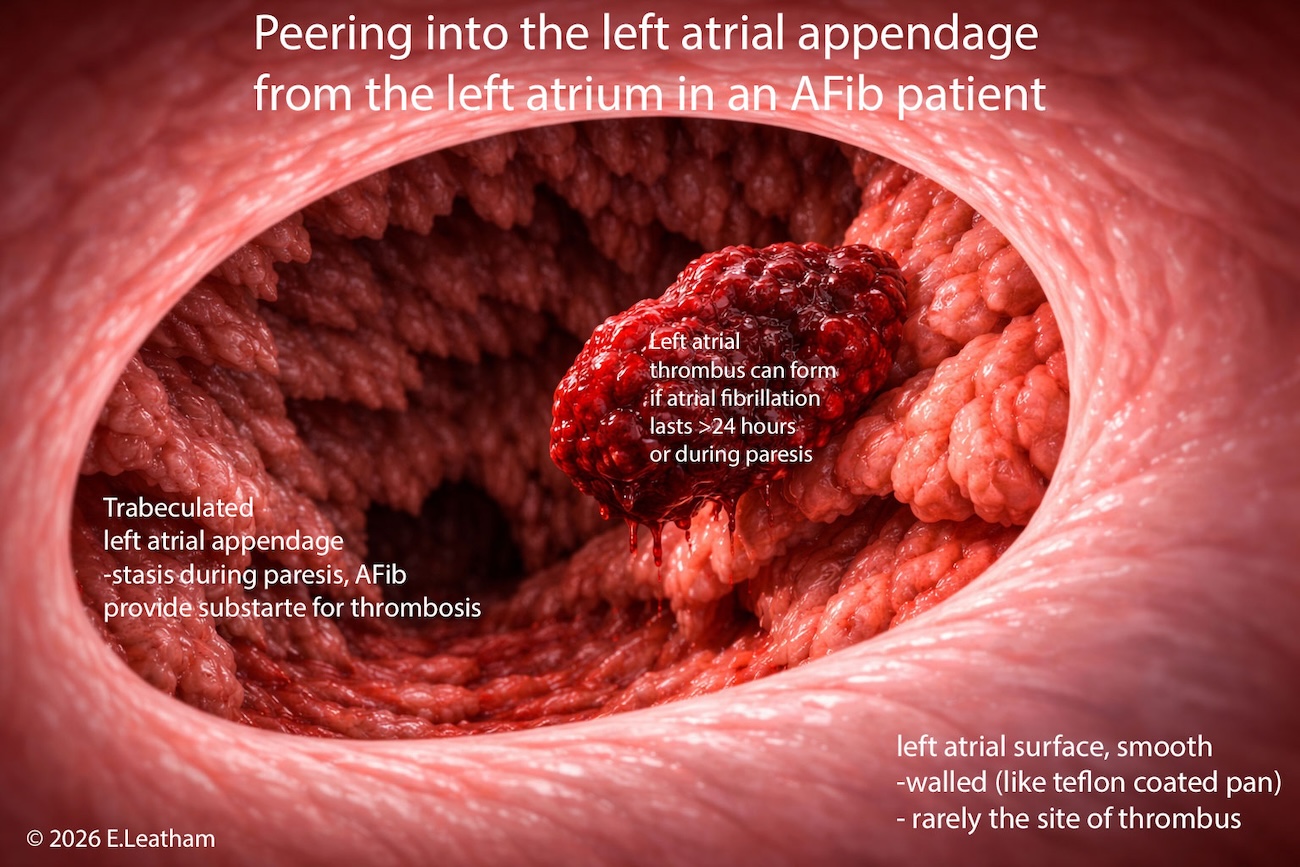
- Clots can form even in 1-2 days or unrecognised episodes
- the natural history of atrial arrhythmias is for increasing frequency and duration over decades
- Some medications eg betablockers and increasing age can mask symptoms so a highly symptomatic patient with PAF can become less aware a decade later, so reliance on symptoms is fallible.
For this reason, guidelines take a safety-first approach.
Where There May Be Room for Individualised Decisions
In carefully selected patients, anticoagulation may not be mandatory—particularly when the clinical picture is very clear.
Possible Exceptions Include:
1. Truly Isolated Episode
- A single, well-documented AF episode
- No recurrence on follow-up monitoring
- Clear trigger (e.g. acute illness, surgery, alcohol)
2. Reliable Rhythm Awareness
- Patient can clearly recognise AF symptoms
- Able to identify onset and termination
3. Short Duration Episodes
- All episodes confirmed to last less than 24 hours
4. Ongoing Rhythm Surveillance
- Regular monitoring using:
- ECG devices (e.g. Preventice monitors)
- Wearables or handheld ECG systems
- Willingness to actively track heart rhythm
5. Informed Patient Choice
- Understanding that:
- Stroke risk is not zero
- Silent AF can occur
- Acceptance of responsibility for monitoring
The Key Clinical Tension
This decision sits between two realities:
Risk of Stroke
- Potentially devastating
- Often unpredictable
- May occur even with minimal or silent AF
Burden of Anticoagulation
- Lifelong medication
- Bleeding risk
- Lifestyle considerations
What Happens Over Time?
An important clinical observation:
- Many patients who initially feel AF clearly
→ Become less aware of it over time
This increases the risk of silent, prolonged episodes, which may shift the balance back toward anticoagulation.
A Practical Approach
For a patient with CHA₂DS₂-VASc ≥2 and a single PAF episode:
Reasonable Strategy May Include:
- Initial period of close rhythm monitoring
- Reassessment for recurrence
- Shared decision-making
Anticoagulation is More Strongly Favoured If:
- AF recurs within a year
- A trend of AFib episodes getting steadily longer over the years
- Episodes last >24 hours
- Monitoring is inconsistent
- Symptoms are unclear or absent
Key Take-Home Message
- Guidelines recommend anticoagulation based on stroke risk, not AF burden alone
- A single episode of PAF does not always mandate lifelong anticoagulation
- However, exceptions apply only in carefully selected, well-informed patients
- Ongoing monitoring and patient engagement are essential
Final Thought
Rather than a rigid “yes or no” rule, this is a shared decision between patient and cardiologist—balancing:
- Stroke prevention
- Treatment burden
- Certainty of rhythm monitoring
Related Blogs
- Two ways AFib can cause stroke or heart attack
- What is Atrial Fibrillation (AFib)?
- Managing your own Atrial Fibrillation: Taking control of your heart health
- How AFib can present as a heart attack or stroke