An article written by Dr Edward Leatham, Consultant Cardiologist © 2025 E.Leatham
Most cholesterol in the blood travels inside protein-based particles called lipoproteins. These include chylomicrons, very low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), low-density lipoproteins (LDL), and high-density lipoproteins (HDL).
All, except HDL, can contribute to the build-up of fatty plaques in arteries — the process known as atherosclerosis.
Traditional cholesterol tests measure how much cholesterol is present by mass. In the UK this is generally reported as total concentration of cholesterol type in serum expressed in mmol/L. Modern tests can be used to measure the number and type of particles carrying that cholesterol.
This option can provide a more accurate picture of cardiovascular risk in some of our patients.
🧪 The NHS “Non-HDL Cholesterol”
In the NHS, the non-HDL cholesterol value is calculated automatically in every lipid profile.
It’s simply:
\text{Non-HDL-C} = \text{Total cholesterol} – \text{HDL cholesterol}
This represents the total amount of cholesterol carried by all the potentially harmful particles — LDL (including sdLDL), VLDL, IDL, and lipoprotein(a).
- It’s a simple and practical measure.
- It correlates well with ApoB, but remains a cholesterol-mass estimate, not a particle count.
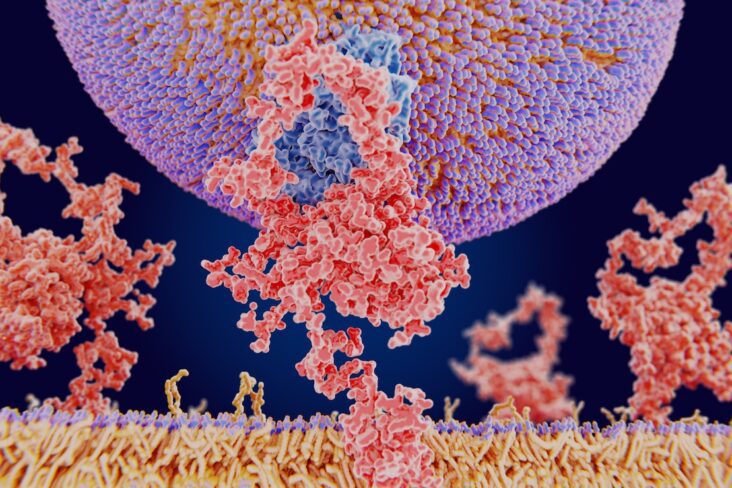
🔬 ApoB — Counting the Particles That Matter
Every atherogenic lipoprotein particle carries one molecule of apolipoprotein B (ApoB).
That means measuring ApoB gives you a direct count of how many cholesterol-carrying particles are circulating in the blood — not just how much cholesterol they contain.
A high ApoB means too many particles, even if your LDL-C number looks normal.
This is particularly common in people with:
- Type 2 diabetes
- Insulin resistance
- High visceral fat (VAT)
- Metabolic syndrome
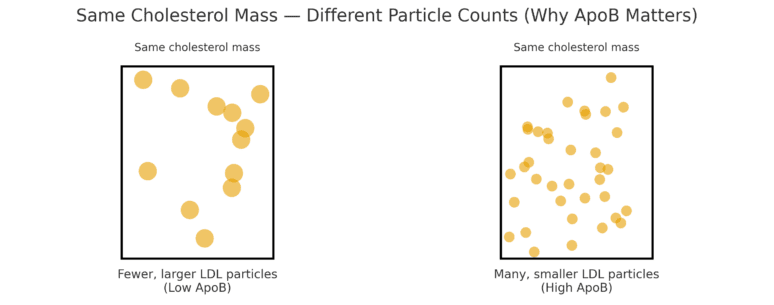
🧩 Why the Number of Particles Matters — Understanding the Image

This picture shows two people who both have the same amount of cholesterol in their blood, but the cholesterol is carried very differently:
Left side: the cholesterol is packed into fewer, larger LDL particles.
Each particle carries plenty of cholesterol, so there are not many particles overall.
→ This person has a lower ApoB level and lower cardiovascular risk.
Right side: the same amount of cholesterol is spread across many smaller LDL particles.
Each particle carries less cholesterol, so the body needs more particles to transport the same total.
→ This person has a higher ApoB level, meaning more smaller particles circulating and greater chance of them entering artery walls.
Even though both have the same total cholesterol, the person on the right has many more opportunities for cholesterol to stick to arteries, increasing long-term risk.
That’s why modern tests such as ApoB — which count the particles — can identify hidden risk that traditional cholesterol tests might miss.
In these states, LDL particles are often smaller and cholesterol-depleted, but more numerous — and it’s the number of small particle LDLs that drives most cardiovascular risk.
⚠️ Small Dense LDL — the Most Dangerous Fraction
Small dense LDL (sdLDL) particles are the most atherogenic type of LDL.
They are:
- Smaller and heavier
- Stay in the bloodstream longer
- More likely to oxidise and enter artery walls
High sdLDL is typical of metabolic syndrome, diabetes, and high triglyceride states linked to visceral fat.
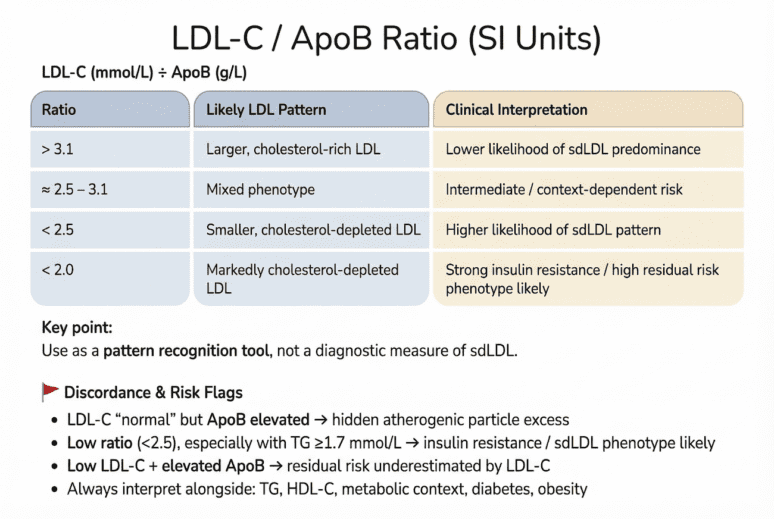
Because sdLDL testing is specialised, the ApoB level and the LDL-C : ApoB ratio can be used to estimate particle size predominance
🇬🇧 Table 1. UK Reference and Risk Ranges for Lipoprotein Markers (Dual Units)
VAT TRAP Copyright 2025 Cholesterol target
Summary of targets:
- Lower targets for higher cardiovascular protection.
- For established CVD ie has had MI/angina/ stent, CAVG/ Cardiac CT showing high risk or high FAI, aim for lower targets:
- LDL-C ≤ 1.4 mmol/L (≤ 70 mg/dL) – aim for even lower, in event of recurrent events
- Non-HDL-C ≤ 2.6 mmol/L (≤ 100 mg/dL)
- ApoB ≤ 0.80 g/L (≤ 80 mg/dL)
🧠 Take-Home Message
- The NHS non-HDL-C test gives a good overall measure of atherogenic cholesterol.
- ApoB adds precision by counting particles, not just measuring cholesterol.
- sdLDL-C and the LDL-C : ApoB ratio reveal particle quality — the difference between large and small LDL.
- Combining these tests gives a clearer picture of cardiovascular risk, especially in people with metabolic syndrome, diabetes, or visceral fat accumulation.
At SCVC we offer blood testing for LDL-C, LP(a) and Apo B in clinic or via a painless test you can run in the comfort of your own home by post. All of our tests are available with or without a cardiologist report.
Use our contact form to make an enquiry or see https://www.scvc.co.uk/your-health-at-home/
References
¹ Heart UK – Understanding your cholesterol test results
² NICE NG238 (2023) – Cardiovascular disease: risk assessment and lipid modification
³ RUH Bath – Lipid management (PATH-018, 2023)
⁴ Synnovis Labs – ApoB Test Information (2024)
⁵ Medscape – Apolipoprotein B Overview (2024)
⁶ Sniderman AD et al. Eur Heart J. 2023;44(21):1930–1944
⁷ Luo J et al. Atherosclerosis. 2024;387:123–132
⁸ Musunuru K et al. J Am Coll Cardiol. 2019;73(12):1610–1623
Related posts and downloads
- Targets for LDL-C, ApoB and Small Dense LDL
- The Hidden Culprit Behind Heart Disease: Small Dense LDL and the Fat You Can’t See