An article written by Dr Edward Leatham, Consultant Cardiologist
1. The Shortcomings of BMI
Body mass index (BMI), defined as weight (kg) divided by height (m²), remains the most widely used measure for obesity classification. However, it is increasingly recognised as inadequate in cardiovascular risk stratification:
- No distinction between fat and muscle: BMI cannot differentiate between lean mass and adipose tissue. Athletes with high muscle mass may be classified as “overweight” or “obese,” while sarcopenic individuals with high visceral fat but low weight may fall into the “healthy” BMI range (1,2).
- Height and frame effects: BMI misclassifies tall, muscular individuals as overweight and underestimates risk in shorter individuals with central adiposity (3).
- Ageing-related bias: Ageing leads to height reduction and sarcopenia, which lowers BMI despite worsening metabolic risk. Thus, BMI may mask true cardiovascular disease (CVD) risk in older adults (4).
2. Visceral Adipose Tissue: The Principal Villain
Visceral adipose tissue (VAT)—fat stored in the abdominal cavity around internal organs—is strongly implicated in cardiovascular and metabolic disease. VAT is metabolically active, secreting pro-inflammatory cytokines (TNF-α, IL-6) and adipokines that promote insulin resistance, dyslipidaemia, hypertension, and atherosclerosis (5).
- VAT measured by CT or DEXA is a strong independent predictor of CVD, type 2 diabetes, and all-cause mortality (6,7).
- Sarcopenic obesity (low muscle, high VAT) is particularly hazardous, combining poor metabolic profile with frailty risk (8).
BMI does not distinguish VAT from subcutaneous fat, nor does it account for sarcopenia—leading to significant misclassification of risk.
3. Waist Circumference and Waist-to-Height Ratio: Better Correlates of VAT
Waist Circumference (WC)
WC reflects abdominal fat distribution and correlates strongly with VAT:
- WC predicts CVD and metabolic risk more accurately than BMI (9).
- Large population studies, such as NHANES III, demonstrated WC to be superior in identifying individuals at risk of metabolic syndrome compared with BMI (10).
Waist-to-Height Ratio (WHtR)
WHtR (waist ÷ height) adjusts WC for stature and has emerged as an even stronger predictor of cardiometabolic risk:
- WHtR consistently outperforms BMI and WC in predicting type 2 diabetes, hypertension, and CVD across sexes, ages, and ethnicities (11,12).
- A WHtR cut-off of 0.5 (“keep your waist to less than half your height”) has been widely validated and recommended in UK public health guidelines (13).
- A meta-analysis confirmed WHtR is superior to BMI for detecting cardiometabolic risk in both children and adults (14).
- Recent prospective data show that individuals with WHtR around 0.65 had a 2.7-fold increased risk of heart failure, independent of BMI category (15).
4. The Muscle Mass Problem: Why BMI Misleads
Sarcopenia (ageing-related muscle loss) lowers BMI despite rising VAT, falsely reassuring clinicians. Conversely, resistance training and increased muscle mass improve insulin sensitivity and cardiometabolic health while raising BMI, wrongly categorising individuals as “overweight” (16).
Thus, BMI penalises muscular individuals and conceals risk in sarcopenic patients. Waist-based measures remain accurate regardless of lean mass variations.
5. Cardiologist’s Perspective: Why Waist Matters
Cardiologists increasingly prioritise WC and WHtR for risk assessment because they:
- Better reflect VAT, the key driver of inflammation and metabolic dysfunction.
- Are unaffected by variations in muscle mass.
- Are inexpensive, reproducible, and applicable across diverse populations.
6. Tracking Progress in Clinical Practice
For lifestyle interventions and pharmacotherapy, waist-based measures provide simple surrogate tracking of VAT reduction:
- Lifestyle interventions: Diet and exercise reduce VAT and improve cardiovascular outcomes. WC is a practical marker of progress (17).
- GLP-1 receptor agonists: These drugs preferentially reduce VAT; thus, WC or WHtR is a valuable measure of efficacy in clinical follow-up (18).
- Advanced imaging: In high-risk patients, DEXA and low-dose CT can directly quantify VAT. DEXA simultaneously assesses muscle mass, enabling detection of sarcopenic obesity (19). CT remains the gold standard, with VAT >100 cm² associated with high risk and >160 cm² with very high cardiovascular risk (20).
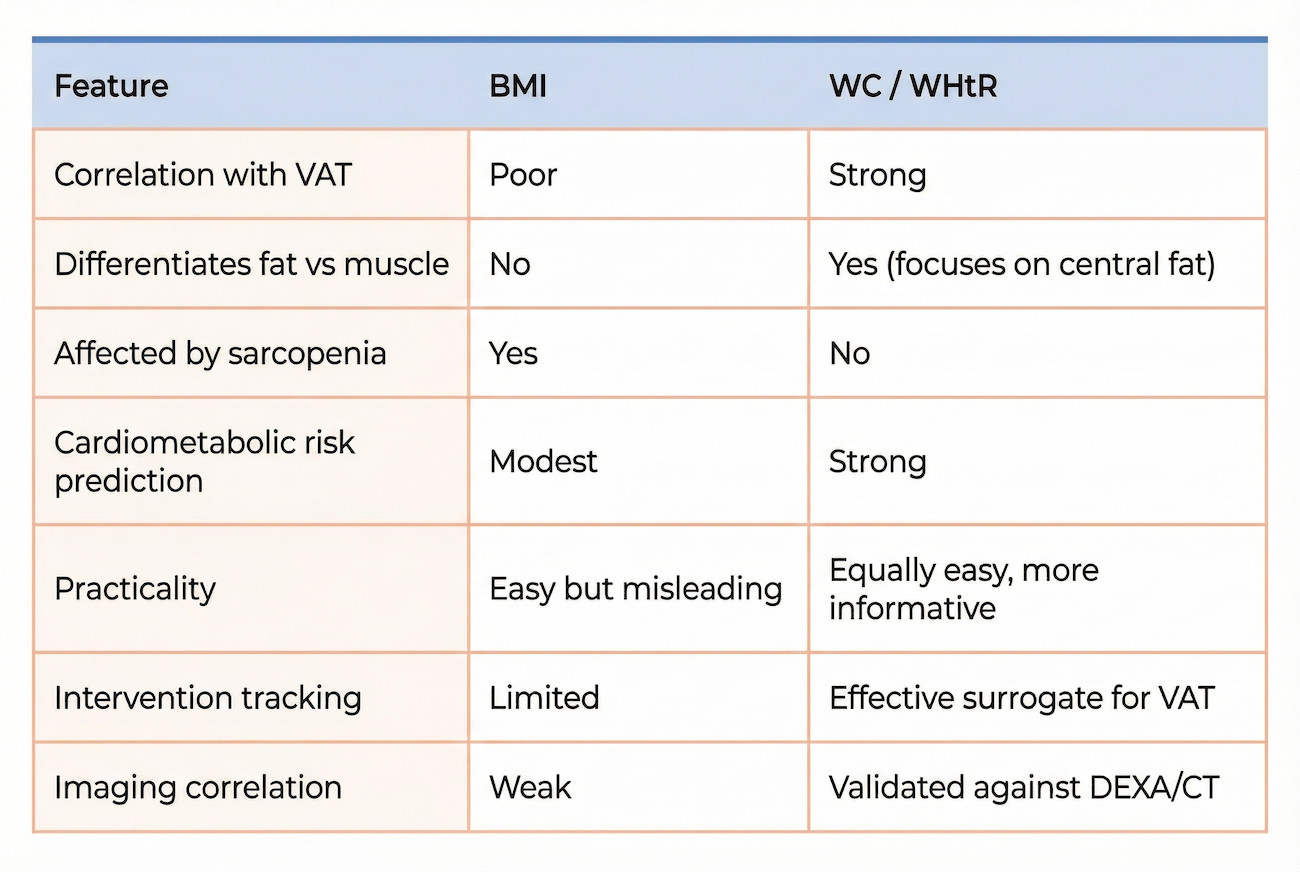
7. Summary Table

8. Conclusion
VAT is the principal metabolic culprit in cardiovascular risk. BMI—while simple—fails to capture fat distribution, muscle mass, or ageing effects. Waist-based anthropometrics, particularly waist circumference and waist-to-height ratio, more closely reflect VAT and strongly predict cardiovascular outcomes.
For cardiologists, this explains why a tape measure around the waist is more valuable than a BMI calculation. Where precise measurement is required—such as in high-risk patients commencing GLP-1 therapy—DEXA and low-dose CT provide direct VAT quantification.
In both prevention and clinical practice, tracking waist measurements makes far more sense than relying on BMI.
References
- Romero-Corral A, et al. Accuracy of body mass index in diagnosing obesity in the adult general population. Int J Obes. 2008;32(6):959-66.
- Rothman KJ. BMI-related errors in the measurement of obesity. Int J Obes. 2008;32 Suppl 3:S56-9.
- Nuttall FQ. Body mass index: Obesity, BMI, and health: A critical review. Nutr Today. 2015;50(3):117–28.
- Kyle UG, et al. Body composition and BMI in elderly subjects. Nutrition. 2001;17(9):731–8.
- Fox CS, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation. 2007;116(1):39-48.
- Després JP. Body fat distribution and risk of cardiovascular disease. Circulation. 2012;126(10):1301–13.
- Neeland IJ, et al. Visceral adiposity and cardiovascular risk: beyond BMI. J Am Coll Cardiol. 2015;66(10):1201–2.
- Prado CM, et al. Sarcopenic obesity: a new category of obesity in oncology? Clin Nutr. 2008;27(5):791–9.
- Janssen I, et al. Waist circumference and not BMI explains obesity-related health risk. Am J Clin Nutr. 2004;79(3):379–84.
- Grundy SM, et al. Prevalence of metabolic syndrome in the US: NHANES III. JAMA. 2004;287(3):356–9.
- Ashwell M, et al. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors. BMJ Open. 2012;2(3):e000650.
- Browning LM, et al. Waist-to-height ratio is superior to BMI and waist circumference for screening cardiometabolic risk in children and adults. Int J Obes. 2010;34(3):418–26.
- National Institute for Health and Care Excellence (NICE). Obesity: identification, assessment and management. NICE Guideline [CG189]; 2014.
- Lo K, et al. Waist-to-height ratio, waist circumference, and BMI as predictors of cardiometabolic risk in children and adolescents: a systematic review and meta-analysis. Obes Rev. 2016;17(12):1257–74.
- Sattar N, et al. Waist-to-height ratio as predictor of heart failure: prospective cohort data. Eur Heart J. 2023;44(29):2711–20.
- Srikanthan P, et al. Muscle mass index as a predictor of longevity in older adults. Am J Med. 2014;127(6):547–53.
- Ross R, et al. Reduction in obesity and related comorbid conditions after diet and exercise. Ann Intern Med. 2000;133(2):92–103.
- Wilding JPH, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989–1002.
- Kaul S, et al. Dual-energy X-ray absorptiometry for body composition: An accurate assessment tool for visceral adiposity. Obesity. 2012;20(6):1313–8.
- Kuk JL, et al. Visceral fat is an independent predictor of all-cause mortality in men. Obesity. 2006;14(2):336–41.
Other related articles
- How to Measure Your Waist
- If You’ve Had a Stent, Check Your Waist
- The Expanding Waistline in Men: Spare Tyre, Killer Visceral Fat, or Just Flabby Abdominal muscles?