The post Why HIIT Gets Rid of Visceral Fat — The Science Behind Anaerobic Exercise appeared first on Surrey Cardiovascular Clinic.
]]>For busy people, or to tune in when on the move, Google Notebook AI audio podcast and an explainer slide show are available for this story beneath.
When patients ask how to “burn belly fat,” what they usually mean is how to lose visceral fat — the deep, internal fat that surrounds the liver, pancreas, and heart. This is the fat that drives inflammation, insulin resistance, and cardiovascular risk.
While many people assume that long, steady aerobic exercise like walking or cycling is the best route to fat loss, evidence increasingly shows that high-intensity interval training (HIIT) — short bursts of near-maximal effort — is one of the most effective ways to reduce visceral adipose tissue (VAT).
Let’s explore why.
1. HIIT Targets the Metabolic Core of the Problem
Visceral fat is not just stored energy — it is a metabolically active organ that releases inflammatory cytokines (IL-6, TNF-α) and free fatty acids directly into the portal circulation. This overloads the liver, impairs insulin sensitivity, and drives a self-reinforcing cycle of fat accumulation.
HIIT interrupts this cycle by dramatically improving insulin sensitivity and glucose uptake in skeletal muscle — particularly in the large lower-limb muscles of the thighs and glutes. A single 20-minute session of HIIT can activate GLUT-4 transporters in muscle cells for up to 24–48 hours, drawing glucose out of the bloodstream and away from storage in the liver and visceral fat depots.
2. The Anaerobic Advantage — Training Without Oxygen
Unlike steady-state aerobic exercise, HIIT operates primarily in the anaerobic zone. During intense effort, oxygen supply can’t keep up with muscle demand, forcing the body to rely on stored glycogen and the phosphocreatine (PCr) system for energy.
This temporary oxygen debt triggers powerful metabolic adaptations:
- Post-exercise oxygen consumption (EPOC): After HIIT, the body consumes extra oxygen for hours to restore energy stores and repair muscle tissue — continuing to burn fat even at rest.
- Hormonal activation: HIIT stimulates adrenaline, growth hormone, and noradrenaline — all potent fat-mobilising hormones that specifically increase lipolysis in visceral fat.
- Mitochondrial biogenesis: Repeated anaerobic stress signals muscles to build new mitochondria, improving the body’s long-term fat-oxidising capacity.
3. Visceral Fat Is More Responsive to Catecholamines
Visceral adipocytes are rich in β-adrenergic receptors, which respond strongly to adrenaline and noradrenaline. These hormones are released during short bursts of intense exercise — precisely what happens in HIIT.
Subcutaneous fat, by contrast, is less responsive. This explains why HIIT preferentially mobilises VAT even when overall body weight changes little. You can “stay the same weight” but still dramatically improve your metabolic profile as visceral fat shrinks and muscle mass increases.
4. HIIT Builds Muscle — and Muscle Is a Fat-Burning Organ
Skeletal muscle is the main site of glucose disposal in the human body. Every gram of additional muscle acts as a metabolic sink for glucose and fatty acids.
HIIT, even in short sessions, preserves and increases lean muscle mass. This is crucial because:
- Muscle raises basal metabolic rate — you burn more energy even while resting.
- Muscle competes with fat for energy supply — reducing the opportunity for visceral fat to expand.
- Muscle improves metabolic flexibility, allowing the body to switch efficiently between glucose and fat as fuel.
In other words, HIIT doesn’t just burn calories during exercise — it changes your physiology so that fat is less likely to return.
5. Short, Sustainable, and Scalable
A major advantage of HIIT is that it can be completed in 10–20 minutes, using nothing more than body weight, resistance bands, or simple movements like squats, push-ups, and sprints.
For busy professionals or older adults, this short-duration, high-reward format improves adherence — and consistency is the ultimate determinant of visceral fat loss.
Even two to three HIIT sessions per week can reduce VAT by up to 20–30% in clinical studies, often outperforming traditional aerobic programs of much longer duration.
6. The Inflammatory Reset
HIIT does more than alter body composition. It resets inflammatory tone. Studies show that reducing visceral fat through HIIT leads to lower high-sensitivity CRP, reduced interleukin-6, and improved endothelial function.
This is why patients often describe feeling “lighter” and “sharper” even before major weight changes appear — the improvement is cellular, not cosmetic.
7. Practical Application — How to Begin Safely
If you’re new to HIIT, start gradually. The goal is intensity, not exhaustion.
A typical starter routine might include:
- 30 seconds of fast effort (e.g. brisk stair climb, cycling sprint, or body-weight squats)
- 90 seconds of active recovery (gentle movement or slow walking)
- Repeat 8–10 times for a total of 15–20 minutes.
Always warm up and cool down. People with known cardiovascular disease or hypertension should discuss new exercise plans with their clinician — HIIT can be safely tailored for all levels, including cardiac rehab, when properly supervised.
8. The Takeaway
HIIT works because it reprogrammes metabolism. It improves insulin sensitivity, activates fat-mobilising hormones, and preferentially burns visceral fat — the type that truly matters for long-term health.
It’s not about chasing calorie counts or spending hours on a treadmill. It’s about stimulating the system — challenging muscle and mitochondria to work harder, recover stronger, and remodel energy use at the cellular level.
In short, HIIT trains your body to burn fat even when you’re not exercising — and visceral fat is the first to go.
Key Takeaways
- Visceral fat is metabolically active and inflammatory.
- HIIT improves insulin sensitivity and glucose uptake in muscle.
- Anaerobic bursts release fat-mobilising catecholamines that preferentially target VAT.
- Muscle gained through HIIT becomes a metabolic buffer against future fat gain.
- 10–20 minutes, two to three times a week, can make a measurable difference.
References
- Maintenance of time-restricted eating and HIIT over 2 years
Design: Randomised/cohort design combining time-restricted eating (TRE) and HIIT interventions.
Findings: After 2 years, participants in HIIT (and TRE + HIIT) had significantly lower body mass, fat mass, and visceral fat area compared to baseline. (Nature) - Effect of eight weeks of HIIT (Iran, PCOS / metabolic population)
Design: 8-week HIIT vs control, in women with PCOS / metabolic syndrome features
Findings: Significant improvements in anthropometric measures (waist circumference, body fat), insulin sensitivity, lipid profile, and inferred visceral fat reduction (via surrogate metrics). (BioMed Central) - “Effect of High-Intensity Interval Training on Visceral and Liver Fat in Cardiac Rehabilitation”
Taylor JL et al. 2020. Obesity (Silver Spring).
Design: Patients with coronary artery disease (CAD) in a 3-month supervised + 11-month home program. They compared HIIT (4×4 min) vs moderate-intensity continuous training (MICT) in their effects on VAT (via MRI) and liver fat.
Findings: Both HIIT and MICT significantly reduced VAT over 3 months (−350 cm³ vs −456 cm³) and maintained further reductions at 12 months (−545 vs −521 cm³). No significant between-group difference in VAT reduction; HIIT tended to yield greater liver fat reduction. (PubMed) - “Effects of various exercise types on visceral adipose tissue in individuals with overweight and obesity: a network meta-analysis”
Chen et al. (2023)
Design: 84 RCTs (n = 4,836) comparing different modalities (moderate aerobic, vigorous aerobic, HIIT, resistance, combinations) on VAT and body composition.
Findings: All exercise modalities (aerobic, resistance, HIIT, combinations) improved VAT, weight, BMI, waist circumference. Among them, vigorous-intensity aerobic and HIIT ranked highest in probability of being most effective at improving VAT. (Wiley Online Library) - “Dose–response effects of exercise and caloric restriction on visceral fat — randomized trial in Chinese women” Design: Randomised controlled trial in overweight Chinese women, testing different HIIT / aerobic protocols and diet intervention arms.Findings: The study demonstrated that a HIIT protocol had a strong effect on abdominal fat reduction (including visceral compartment) beyond caloric restriction alone, supporting a dose–response relation. (British Journal of Sports Medicine)
- “Comparative Efficacy of Exercise Type on Visceral Adipose Tissue” (recent meta-analysis) Design: Systematic review and meta-analysis comparing different exercise types (continuous training, HIIT, resistance, etc.) for effects on visceral fat. Findings: Concludes that continuous training (CT) had the highest ranking (P-score) in effectiveness, but HIIT still performed favorably; the authors caution interpretation depends on protocol, duration, and population. (Wiley Online Library)
Related posts
- Intervention programmes: from self-toolkits to nurse-led escalation to GLP-1 support
- Cardiometabolic toolkit
- Visceral Fat, Mitochondria, and the Energy Trap: Why We Store Fat Where We Shouldn’t
- Carbohydrate Sensitive Phenotype (CSP): Precursor of the Metabolic Syndrome?
- Exercise and Digital Tools Should Be the First Line in Reducing Visceral Fat in Cardiac Patients
- Cardiologists and a New Enemy: Evolving Tools of the Trade
- Carbohydrate Sensitive Phenotype (CSP): Precursor of the Metabolic Syndrome?
- Metabolic Health Assessment
- Biofeedback: CGM metrics improve after just 4 weeks of dietary intervention
- Lets compare continuous glucose monitor (CGM) results
The post Why HIIT Gets Rid of Visceral Fat — The Science Behind Anaerobic Exercise appeared first on Surrey Cardiovascular Clinic.
]]>The post Exercise and Digital Tools Should Be the First Line in Reducing Visceral Fat in Cardiac Patients appeared first on Surrey Cardiovascular Clinic.
]]>Introduction
Visceral adipose tissue (VAT) is a pro-inflammatory, metabolically active fat depot that plays a key role in the pathogenesis of hypertension, coronary heart disease (CHD), and atrial fibrillation (AF). Unlike subcutaneous fat, VAT resides deep within the abdomen and contributes to insulin resistance, endothelial dysfunction, and adverse cardiac remodelling¹.
Traditional risk markers like BMI fail to capture VAT burden. Instead, VAT index (VATI)—the VAT area in cm² indexed to body surface area (m²)—offers a precise, clinically meaningful target. Our practice applies gender- and ethnicity-specific VATI thresholds, such as <38 cm²/m² for Caucasian men and <28 cm²/m² for Caucasian women, with lower thresholds for Asian populations².
1. Screening with Waist-to-Height Ratio
The waist-to-height ratio (WHtR) is a simple and effective tool to flag individuals at higher risk of VAT accumulation. A WHtR ≥ 0.5 indicates increased cardiometabolic risk, even in patients with normal BMI³.
Why use WHtR ≥ 0.5?
- More accurate than BMI for central fat
- Quick, reproducible, and cost-free
- Valid across age, sex, and ethnic groups
- Especially valuable in identifying VAT in patients with non-diabetic hyperglycaemia (NDH)—defined as impaired fasting glucose or impaired glucose tolerance⁴
2. VATI Requires Imaging for Precision
Waist-to-height ratio is a better guide to VAT than BMI, but it still reflects both subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT). SAT is metabolically inert; VAT is inflammatory and strongly linked to cardiometabolic risk⁵. The waist circumference is a valuable tool to monitor changes in central adiposity over time. However, it cannot distinguish VAT from SAT. Therefore in order to accurately identify and track VAT, an imaging test—such as low-dose CT or MRI— may be essential. We use low-dose, single-slice CT at L3, which is:
- Highly reproducible
- Low in radiation
- Cost-effective for long-term monitoring⁶
For selected patients at risk, we establish baseline VATI assessment with an option for repeat assessment at 6 months, which supports decision-making around therapy escalation (e.g. GLP-1 receptor agonists) and validates response to lifestyle change.
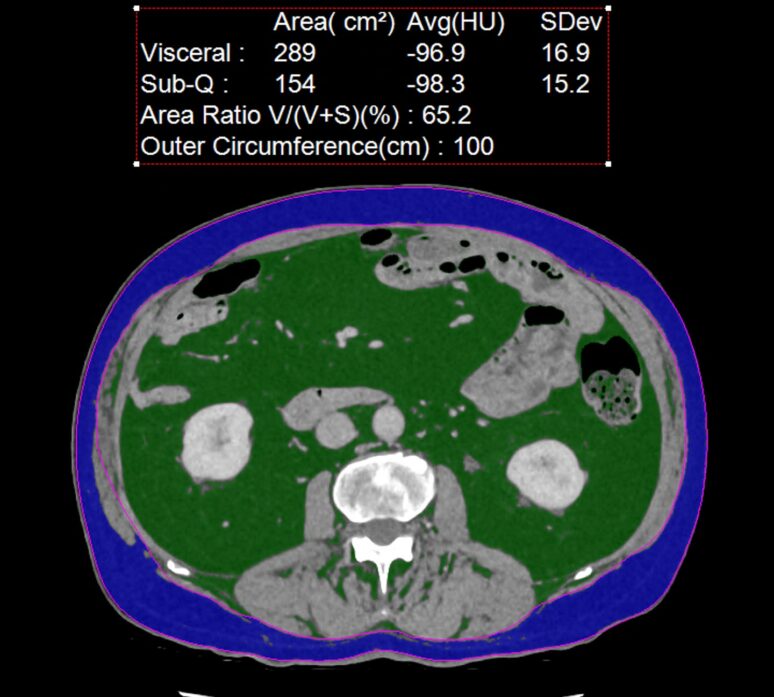
An example of a non contrast CT showing visceral adipose in green and metabolically inactive subcutaneous adipose tissue in blue. In this patient the VAT measures 289 cm2 which is over double recommended (100 cm2).
3. VATI Targets by Gender and Ethnicity
Using gender- and ethnicity-specific VATI thresholds improves sensitivity and specificity in identifying high-risk individuals:
| Ethnicity | Male VATI Threshold (cm²/m²) | Female VATI Threshold (cm²/m²) |
|---|---|---|
| Caucasian | <38.0 | <28.0 |
| South Asian | <34.0 | <25.0 |
| East Asian | <32.0 | <23.0 |
| Black | <36.0 | <26.0 |
| Hispanic | <36.0 | <27.0 |
| Other/Unspecified | <35.0 | <26.0 |
4. Digital Tools as Adherence Amplifiers
Lifestyle change works—but long-term success depends on adherence. Our program uses structured digital tools and personalised planning frameworks to support this journey.
1. Dr Shape Food Analysis App
Our patients are enrolled in Dr Shape, a clinical nutrition app programmed with their personal calorie and macronutrient goals. It acts as a real-time food bot, providing:
- Meal-by-meal feedback
- Macronutrient breakdowns and adjustments
- Goal tracking across the day
- Behavioural nudges to improve food choices
Patients use Dr Shape daily for at least 3 months, allowing precise, data-driven dietary guidance outside clinic settings.
2. Continuous Glucose Monitoring (CGM)
Used to identify those affected and to treat patients with non-diabetic hyperglycaemia (NDH) or insulin resistance, CGM is used to:
- Identify post-meal glucose excursions
- Tailor carbohydrate intake and timing
- Help prevent hyperglycaemia-driven VAT accumulation
3. Body Composition Scales and Waist Tracking
We encourage use of smart body composition scales to monitor:
- VAT estimates (where available)
- Lean mass retention
- Hydration status
Paired with weekly waist circumference, these tools help patients track their own progress and reinforce motivation between imaging assessments.
4. Optional Nutrigenomix DNA Testing
For selected patients—particularly those with metabolic resistance or micronutrient concerns—we offer Nutrigenomix DNA testing. This test identifies gene variants that affect:
- Protein requirements
- Lactose or fat sensitivity
- Caffeine metabolism
- Micronutrient metabolism (e.g. folate, B12, vitamin D)
This information helps tailor the dietary plan even further—e.g., lowering daily protein targets or advising folate-rich foods in those with MTHFR variants.
5. Tiered 6-Month VATI Intervention Pathway
Tier 1: Digital Lifestyle Program (First 6 Months)
Patients with VATI above target are invited to enter a 6-month lifestyle and dietary programme, gradually incorporating the following into a long term, sustainable lifestyle changes:
- Aerobic activity ≥150 mins/week
- Resistance training 2x/week or daily 10 min routine.
- HIITS 10-15 min 3 x each week
- Caloric targets with macronutrient goals via Dr Shape
- Digital adherence tools (CGM, smart scale, waist tracking)
After 6 months, VATI can be re-assessed via repeat CT or surrogate.
Tier 2: Add GLP-1 Receptor Agonist (If Target Not Met)
For non-responders (VATI remains ≥ threshold), or where there is a strong preference to intervene, GLP-1 receptor agonists are added:
- Proven to reduce VAT independently of weight loss⁷
- Improve insulin sensitivity and reduce hunger
- Recommended in high-risk patients by expert guidelines⁸
6. Follow-Up and Reassessment
Every 6 Months:
- CT VATI measurement
- Waist circumference and weight
- Smart scale body composition metrics
- (If hypertensive)
BP via Hilo BP band
- CGM in NDH patients
This structured follow-up ensures we track metabolic progress and tailor therapy only where needed.
Conclusion
VAT reduction is a clinically powerful and achievable goal. Our programme identifies high-risk patients using WHtR and imaging, and applies a tiered model of care centred around:
- Digital dietary support (Dr Shape)
- Real-time glucose tracking (CGM)
- Smart scales and waist tracking
- 6-month imaging reassessment
- GLP-1 therapy only in non-responders
This approach empowers clinicians and patients alike—delivering precision, avoiding overtreatment, and improving cardiometabolic outcomes.
References
- Fox CS, Massaro JM, Hoffmann U, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors. Circulation. 2007;116(1):39–48.
- Ashwell M, Gibson S. Waist-to-height ratio is a simple and effective screening tool for cardiovascular risk. Obes Rev. 2016;17(3):275–86.
- Alberti KG, Zimmet PZ. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia. Diabet Med. 1998;15(7):539–53.
- Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–8.
- Shen W, et al. Estimating body composition from a single CT image. Am J Clin Nutr. 2004;80(2):271–8.
- Baggerman MR, et al. Reference values for visceral fat by CT. Obesity (Silver Spring). 2023;31(1):12–21.
- Oh TJ, et al. GLP-1 RA and SGLT-2 inhibitors in VAT reduction. PLoS One. 2023;18(9):e0289616.
- Yum Y, et al. Expert consensus on hypertension management in obesity. Clin Hypertens. 2024;30(1):13.
Other related articles
- Anthropometrics vs BMI: Why Waist Measures Outperform BMI in Cardiovascular Risk Assessment
- Why everyone is talking about VAT
- How to Lose Visceral Adipose Tissue (VAT) and Improve Metabolic Health: A Guide to Sustainable Weight Loss
- The Expanding Waistline in Men: Spare Tyre, Killer Visceral Fat, or Just Flabby Abdominal muscles?
- From Genes to Greens: How DNA Shapes Your Nutritional Needs
- The 8-Month Metabolic Reset: A New Approach to Reversing Visceral Fat, Improving Blood Pressure and Blood Glucose
The post Exercise and Digital Tools Should Be the First Line in Reducing Visceral Fat in Cardiac Patients appeared first on Surrey Cardiovascular Clinic.
]]>