
Measuring your blood pressure at home
It is important that your blood pressure is well controlled, and low enough to prevent long term damage to the circulation.
Providing independent clinical excellence since 2005
Posted on Wednesday April 24, 2024 in Cholesterol & Atherosclerosis
An article written by Dr Edward Leatham, Consultant Cardiologist © 2024 E.Leatham
In the realm of cardiovascular health, awareness about cholesterol levels and their effects on the body is relatively widespread. However, a specific type of lipoprotein known as Lipoprotein(a), LPA or Lp(a) remains under explored and under appreciated, despite its significant implications for coronary heart disease (CHD). This article highlights the defect that explains why people who inherit the gene coding for high LP (a) may be at greater risk of heart attacks or strokes, even if they appear perfectly healthy, with the objective of raising awareness of the emerging role of Lp(a) as an important cardiovascular risk factor, that may be worth measuring.
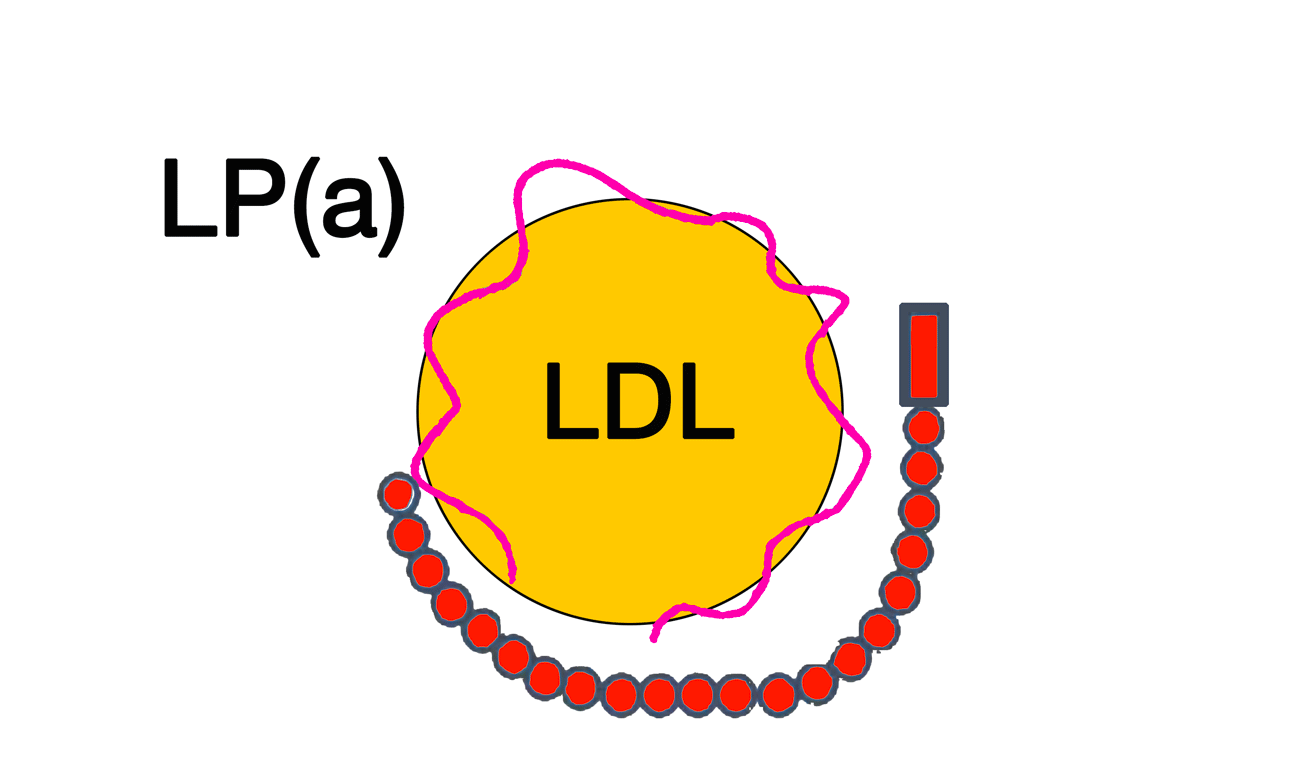
While most are familiar with low-density lipoprotein (LDL) or “bad” cholesterol, fewer are aware of the dangers posed by Lp(a). Research indicates that up to 20% of the global population might have elevated levels of Lp(a), significantly increasing their risk of heart attacks and other severe cardiac events. Lp(a) consists of LDL cholesterol linked to a protein called apolipoprotein(a), which makes it more likely to cause arterial blockages and clots.
Despite its role, Lp(a) is seldom measured in routine checks and often goes unnoticed by even the most diligent cardiologists, mainly due to its complex nature and the limited treatment options currently available. Within a few months of including the LP (a) test as part of our metabolic health assessment for patients with high FAI scores (indicating much higher risk of fatal coronary events within 8 years) undergoing an individualised approach to CHD prevention, we have discovered numerous patients have high LP(a): another poignant example of the old saying that ‘the more you look, the more you will find’.
The first and perhaps the most well-understood mechanism is through its similarity to other apolipoprotein B (ApoB)-containing lipoproteins. Like LDL and other members of the ApoB family, Lp(a) can penetrate the arterial wall. Once inside, it promotes inflammatory reactions, a pivotal step in the pathogenesis of atherosclerosis. The presence of Lp(a) in the arterial wall facilitates the accumulation of lipids and inflammatory cells, leading to plaque formation. These plaques can progressively narrow the arteries, reduce blood flow, or rupture, leading to serious cardiovascular events such as heart attacks and strokes.
Lp(a) is also a significant carrier of oxidized phospholipids (OxPLs), which have been directly implicated in the development of cardiovascular disease. Studies have shown that blood levels of OxPLs are strongly associated with the risk of atherosclerotic disease. OxPLs contribute to the atherogenic process by promoting inflammation, endothelial dysfunction, and further oxidative damage within the arterial wall. Additionally, OxPLs carried by Lp(a) have been associated with an increased risk of calcified aortic valve stenosis, highlighting another pathway through which Lp(a) may lead to cardiovascular complications.
The unique structure of Lp(a), especially the apolipoprotein(a) component, bears a striking resemblance to plasminogen, an enzyme crucial for the dissolution of blood clots. This structural similarity suggests that Lp(a) might competitively inhibit the function of plasminogen. By interfering with the natural fibrinolytic (clot-dissolving) process, high levels of Lp(a) could potentially increase the risk of thrombosis, further complicating its role in heart disease. This mechanism suggests a dual threat posed by Lp(a) – not only does it contribute to atherosclerosis, but it may also exacerbate the risk of acute thrombotic events.
Historically, Lp(a) was only considered a concern in conjunction with other cardiovascular risk factors. However, it is now recognized as an independent risk factor for heart disease, affecting even young, seemingly healthy individuals. High-profile cases, such as Emmy-Award-nominated actress Marin Hinkle and Sandra Tremulis, founder of the Lipoprotein(a) Foundation, who discovered a 95% blockage at age 39, highlight the insidious nature of high Lp(a) levels.
The level of Lp(a) in individuals is primarily determined by genetics, specifically the LPA gene. This makes traditional preventive strategies like diet and exercise ineffective in reducing Lp(a) levels. It also underlines the importance of genetic factors over lifestyle in managing this risk factor. Further complicating matters are the racial disparities in Lp(a) levels, with Black individuals generally having higher levels than other races, necessitating more research into the role of genetics and ethnicity.
Interestingly, Lp(a) can significantly impact the overall levels of LDL cholesterol measured during standard blood tests. For instance, individuals with high Lp(a) might show deceptively high LDL-C levels, which could skew their cardiovascular risk profile if Lp(a) is not separately measured. This makes Lp(a) testing worthwhile, particularly for those who continue to experience cardiovascular events despite having controlled LDL levels.
Understanding your Lp(a) level is important for a comprehensive assessment of cardiovascular risk. This lipoprotein can carry a substantial portion of your LDL cholesterol, potentially increasing your risk of heart disease and stroke beyond what standard cholesterol tests might suggest. Lp(a) testing is therefore advised for individuals at high risk for cardiovascular disease, including those with a prior stent or bypass operation, coronary syndrome or heart attack as well as anyone with a family history of coronary heart disease, high FAI (coronary inflammation) or high risk patterns on Cardiac CT angiograms. In our practice, Lp (a) is offered as part of our comprehensive Metabolic Health assessment (MHA1).
Here’s how Lp(a) levels are typically categorised in terms of cardiovascular risk:
It should be noted that high risk does not mean all people affected will develop a heart condition, only that they are more likely in comparison to ‘low risk’, so Lp(a) is a cardiovascular risk factor similar to smoking, diabetes and high LDL cholesterol.
Studies on the effect of diet on Lp(a) levels are limited. However, low-fat diets, in particular, seem to result in a small but significant increase in Lp(a) whereas a low-fat, high-carbohydrate diet may increase Lp(a) levels compared to a high-fat, low-carbohydrate diet. Currently, no licenced treatments specifically target Lp(a) levels. Common cholesterol-lowering drugs like statins do not affect Lp(a) levels and might even increase them. Some evidence suggests that niacin can reduce Lp(a) levels, but it is not approved for this use, and its effectiveness in reducing cardiovascular risk remains unproven. New therapies are currently being tested in trials for example the HORIZON phase III trial is investigating the benefit of Lp(a)-lowering with an antisense oligonucleotide (ASO), TQJ230, compared to placebo, on major cardiovascular endpoints.
Studies on the effect of diet on Lp(a) levels are limited. However, low-fat diets, in particular, seem to result in a small but significant increase in Lp(a) whereas a low-fat, high-carbohydrate diet may increase Lp(a) levels compared to a high-fat, low-carbohydrate diet. Statins can both raise and lower Lp(a)levels. Niacin decreases Lp(a) levels by approximately 20%-30% and PCSK9 inhibitors lower Lp(a) by upto 30%. Recently, Lp(a)-specific lowering medications have become available and major ongoing clinical trials are investigating the clinical efficacy of these agents in patients with elevated Lp(a) levels: for example the HORIZON phase III trial is investigating the benefit of Lp(a)-lowering with an antisense oligonucleotide (ASO), TQJ230, compared to placebo, on major cardiovascular endpoints.
At SCVC, we now offer a database of patients with coronary heart disease that have raised LP (a), so that we can update any of those interested as soon as new medical therapies become available. Until then, most consultants manage raised LP (a) by treating other risk factors that contribute to cardiovascular risk, such as raised LDL, unhealthy lifestyle, diets and anti inflammatory drugs such as colchicine to mitigate risk. For those found to be at apparently extremely high risk of future heart attack (discovered by undergoing a detailed CT study that includes an assessment of coronary artery inflammation (FAI)), once the subgroup affected by raised LP (a) are identified, we discuss the option of a rescan after 2-3 years of standard preventative therapy, in order to find those we believe may be at high residual risk. These patients would be obvious candidates to offer the option of latest antisense drugs to, if and when they become generally licenced and available.
Lp(a) stands out as a significant, yet often overlooked player in cardiovascular health. With its significant genetic component and its ability to independently elevate cardiovascular risk, understanding and managing patients with raised Lp(a) levels is increasingly important. As research advances and new treatments are developed, the hope is that more light will be shed on this stealthy risk factor, leading to better prevention strategies and outcomes for those at risk. Awareness and education about Lp(a) are key, as they are the first steps towards tackling this hidden threat to heart health.
It is important that your blood pressure is well controlled, and low enough to prevent long term damage to the circulation.
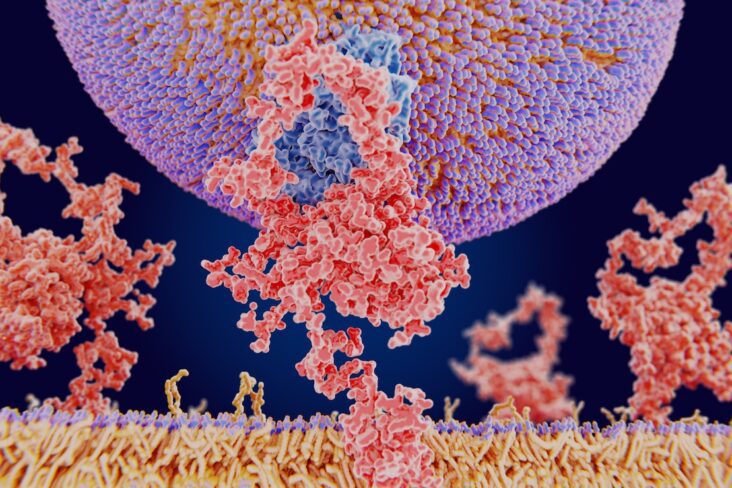
PCSK9 binds to LDL receptors and directs them to be destroyed within the cell, rather than allowing them to recycle to the surface. When too much PCSK9 is present, fewer LDL receptors remain available to clear LDL from the blood. The result is simple: LDL levels rise. When that happens, the liver compensates by making even more cholesterol internally. This is why around 90% of the cholesterol in your blood is made by your liver, not absorbed from your diet.

An article by Dr Edward Leatham, Consultant Cardiologist © 2024 E.Leatham For busy people, or to tune in when on the move, Google Notebook AI audio podcast are available for this story beneath. Introduction Pulse rate or heart rate is a fundamental […]