An article by Dr Edward Leatham, Consultant Cardiologist
As one of the training registrars working at the London Chest Hospital in Hackney, East London, we once spent most of every weekday in the cath lab undertaking invasive coronary angiograms and PCI. At the time, EBCT to measure coronary calcification to predict future heart attack risk was something we read about but had no practical experience of. Coronary calcification was understood, in interventional terms, as something that made angioplasty more difficult, since calcified plaque was harder to ‘crack’ with a balloon inside the vessel. We often had to exceed the rated burst pressure on high-pressure angioplasty balloons to succeed in widening the diseased coronary vessel sufficiently to fit a stent. When viewing an angiogram of a patient with very heavily calcified coronary arteries, ‘RB’, our senior and wisest of all cardiologists, would say, “and there is God’s stent.” Nearly three decades on, he may turn out to have been right!
A local fundraiser once asked me whether he should have a coronary artery calcium (CAC) score. He was 83 years old and was already on high-dose statins and a junior aspirin, so I replied that it wouldn’t alter management, so it was probably not worth doing. He ignored my advice and then sent me a panicky email one Christmas day to say he had received his results by post the day before. The report alarmed him, as his CAC was exceedingly high (>2000), and for sure, his coronary arteries were heavily calcified. The patient imagined that this meant he was about to have his last Christmas and would be in need of an urgent invasive angiogram! He did eventually have an invasive angiogram, which confirmed calcified, non-obstructive coronary artery disease. He went on to live 15 years without ever having angina or requiring a stent. The point of this story is that the presence of coronary calcification does not necessarily imply high risk; the context matters.
Understanding Coronary Artery Calcification
Coronary artery calcification is a marker and not the cause of coronary plaque; however, we now understand it to be part of the body’s natural healing response to inflammation. CAC is common in men over 60 and women over 70. While there is certainly a correlation between the extent of CAC and future risk, its absence does not exclude coronary plaque. If anything, non-calcified plaque is potentially more dangerous than calcified plaque, as heart attacks and sudden death are caused by the rupture of soft (non-calcified) plaque, not generally by heavily calcified plaque. The exception is where the outside shell of a plaque has calcified (so it cannot expand outward radially), and a pool of soft or liquid plaque is present between the calcified plaque and the blood vessel. Here, shear force can be more directly applied, rupturing the fibrous cap and allowing the lipid-rich pool to come into contact with circulating platelets, initiating coronary thrombosis.
The Evolution of CT Technology
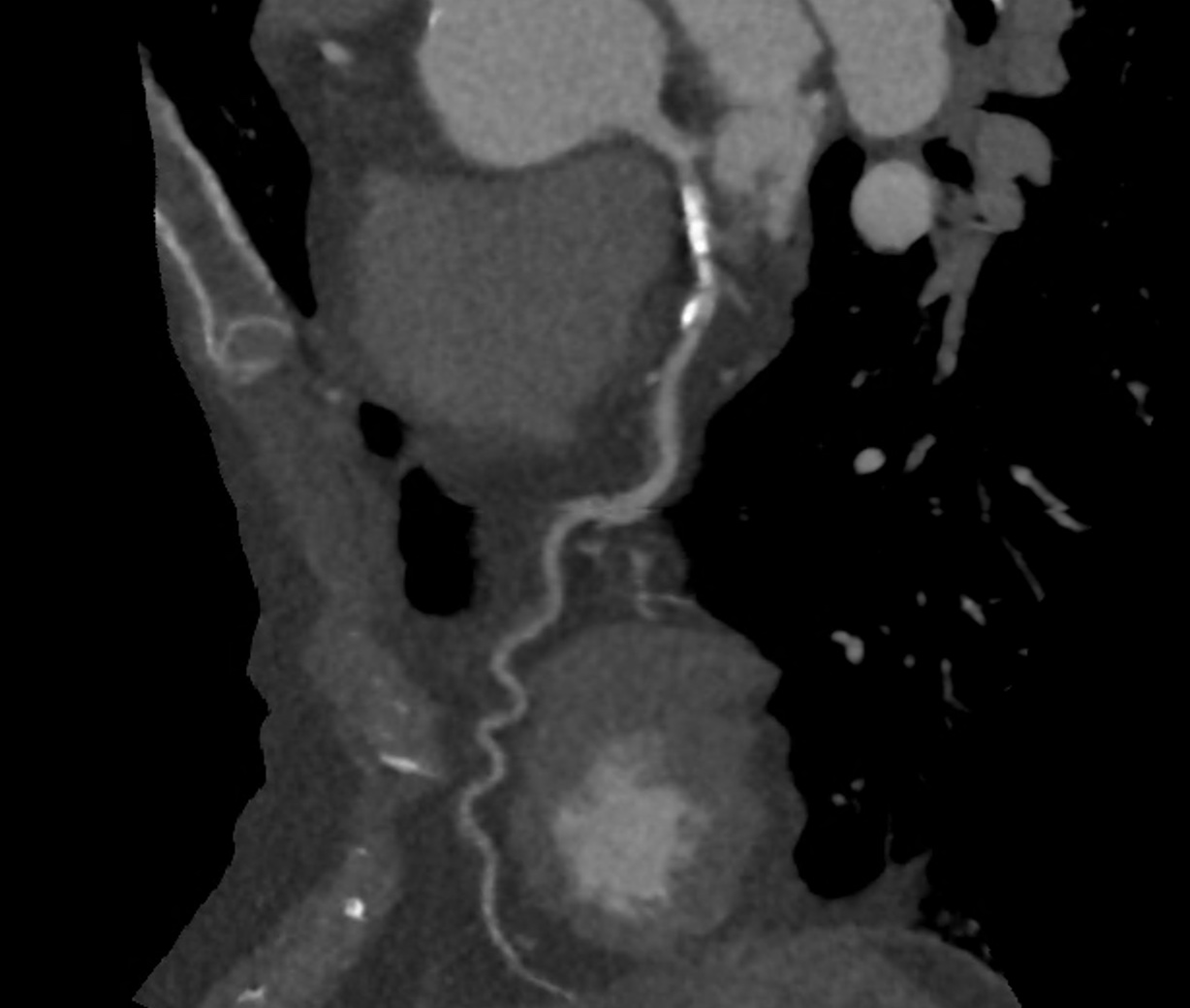
With the advent of multi-slice CT (MSCT), lower doses of radiation, and more medical interventions available to treat coronary disease, cardiologists are increasingly using CTCA to track the course of the disease particularly in higher-risk patients. It is now sometimes possible to observe changes in the same vessel of the same patient a few years apart. In the example shown below, the right coronary artery is affected close to its origin by non-calcified plaque, seen as an indentation in the vessel wall at the blue cross mark. The cross-sections are shown beneath, allowing comparison of diseased versus healthy sections (red cross mark). The indentation is caused by a crescentic atheromatous plaque, with low grayscale density, signifying soft or non-calcified plaque.
The Role of Statins in Plaque Calcification
The figures below show the same patient’s right coronary artery after three years of taking statins. The plaque is still present; however, its volume is similar, and the density has changed to being ‘white,’ meaning that some of the plaque has calcified. This case illustrates the latest thinking, which is that the goal of modern prevention is to both prevent atheromatous plaque from developing and, once present, to accelerate the hardening and calcification of any soft or non-calcified plaque by prescribing statins. These drugs have multiple effects, the principal one being to lower LDL.

The same patient and artery after taking statin each day for 3 years.
Case Study and Modern Practices
In modern cardiology practice, the shift towards using advanced imaging techniques like MSCT has allowed us to provide more comprehensive care. In this single case, the patient’s right coronary artery showed significant non-calcified plaque. After three years of statin therapy, follow-up imaging showed that the plaque had begun to calcify, indicating a stabilising response.
This supports the modern approach that emphasises not just preventing plaque formation but also encouraging the calcification of existing soft plaques. Statins play a crucial role in this process, helping to lower LDL levels and promote plaque stability through calcification.
Conclusion
In conclusion, coronary artery calcification, once seen as a challenge in interventional cardiology, is now understood as a protective mechanism. While it is an indicator of existing coronary artery disease, it also signifies the body’s efforts to stabilise potentially dangerous plaques. For patients with coronary artery disease, the goal is to transform soft, vulnerable plaques into hardened, calcified ones that are less likely to rupture and cause acute events.
As our understanding of coronary artery disease evolves, so too does our approach to its management. Calcification of coronary plaques, aided by treatments like statins, is now a desired outcome in the prevention of heart attacks and sudden cardiac death. This shift in perspective underscores the importance of personalised, evidence-based strategies in the management of coronary artery disease.
Understanding and embracing this new paradigm can significantly improve long-term outcomes for patients, ensuring they live healthier, longer lives.
Further Reading